Endolymphatic Sac Decompression
Main Text
Table of Contents
Abstract
Endolymphatic sac (ELS) decompression can be performed for patients with Meniere’s disease who have failed conservative treatment such as dietary changes and medical therapy. The full pathophysiological mechanisms that result in Meniere’s disease are not entirely understood. The variation in techniques for performing ELS decompression support this; there is no concrete data to justify one approach over another. Regardless, in the correct patient, ELS decompression can significantly alleviate the patient’s symptoms. To do so, a mastoidectomy is performed to expose the bony labyrinth as well as the bone overlying the sigmoid sinus. Decompression of the sac can be accomplished by removing overlying bone, incising the dura, or stenting the dura open.
Case Overview
Background
The clinical symptoms of Meniere’s disease include fluctuating-progressive hearing loss, episodic vertigo, tinnitus, and aural fullness.1 These symptoms are thought to be a result of increased endolymphatic fluid, which distorts the membranous labyrinth, though the exact mechanisms of such are poorly understood.
Focused History of the Patient
In this case, a 68-year-old patient presented with vertigo episodes associated with fullness and pressure in the left ear, as well as tinnitus and decreased hearing. He had attempted dietary changes as well as medical treatment with a diuretic and oral steroids. Although oral steroids made improvements in hearing, these dosages could not be maintained safely. He also had several rounds of steroid injections into the middle ear space that provided slight improvement in his hearing and relief of his vertigo episodes. Over several years, however, his symptoms became resistant to steroid injections as well as short courses of oral steroids. He also developed symptoms related to the right ear.
Physical Exam
There were no abnormal findings on his otoscopic exam. His tympanic membrane was normal in appearance without evidence of retraction or middle ear effusion.
Adjunctive Studies
Vestibular testing demonstrated abnormal findings on his vestibular-evoked myogenic potentials (VEMP). His ocular VEMP responses are present but with amplitude asymmetry that is worse in the left ear. His audiogram at presentation shows that tympanometry is normal bilaterally and that his left ear has moderate to moderate-severe sensorineural hearing loss with a speech reception threshold of 55 dB and a speech discrimination of 56% (Fig. 1). After a year of symptom fluctuation and treatment with steroids (both oral and intratympanic) and diuretics, his audiogram revealed bilateral moderate-severe sensorineural hearing loss (slightly worse in the lower frequencies) with a speech reception threshold of 55 dB in the right ear and 60 dB in the left ear and speech discrimination of 76% in the right ear and 64% in the left ear (Fig. 2).
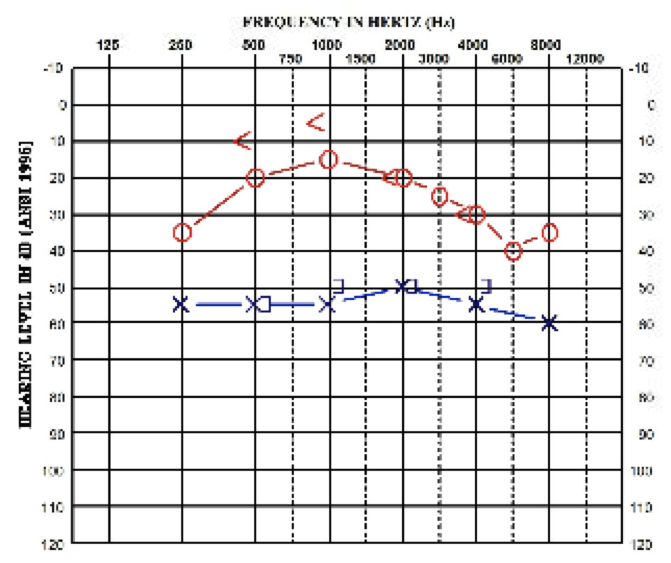 Fig. 1, Audiogram at presentation (x-axis is Frequency in Hz, y-axis is Hearing Level / Intensity of the Sound in dB). The left ear is denoted by blue.
Fig. 1, Audiogram at presentation (x-axis is Frequency in Hz, y-axis is Hearing Level / Intensity of the Sound in dB). The left ear is denoted by blue.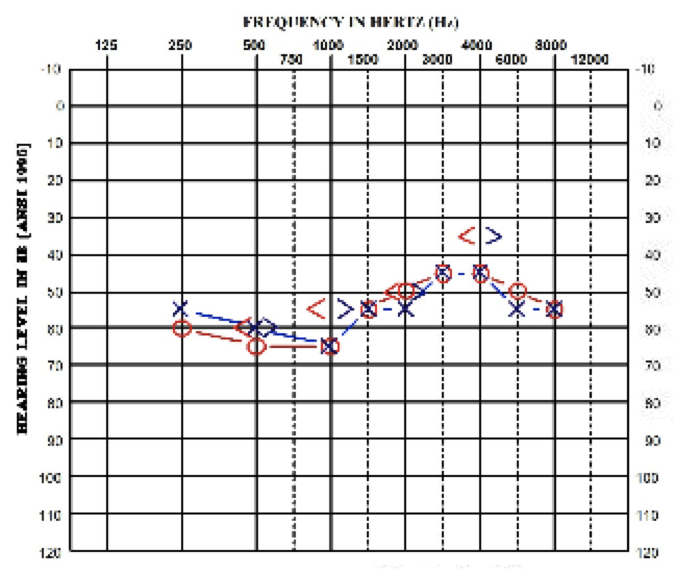 Fig. 2, Audiogram one year after presentation (x-axis is Frequency in Hz, y-axis is Hearing Level / Intensity of the Sound in dB). The left ear is denoted by blue.
Fig. 2, Audiogram one year after presentation (x-axis is Frequency in Hz, y-axis is Hearing Level / Intensity of the Sound in dB). The left ear is denoted by blue. Natural History
Meniere’s disease may be difficult to diagnose due to the fluctuating nature of symptoms as well as the lack of any definitive testing for diagnosis. It has an episodic course, and certain patients may undergo spontaneous remission of their vertigo.2 Although the hearing loss in Meniere’s disease is typically described as fluctuating, there may also be a gradual overall decline in a patient’s hearing levels, even in the absence of other symptoms such as aural fullness or vertigo. Overall, prolonged disease may cause deterioration of hearing, and intense tinnitus is more often seen in the later stages of the disease.3
Options for Treatment
Surgery for Meniere’s disease is typically not the first option or course of treatment, and there are multiple surgical methods that can be performed. To understand the possible treatment modalities, it is important to grasp the underlying pathophysiology of the condition. The hydropic state of the inner ear has been confirmed in temporal bone studies and is described as the primary pathologic mechanism in Meniere’s disease.4 Therefore, treatments will target pathways that can influence the degree of hydrops that is present.
At the least invasive end of the spectrum, dietary changes such as the reduction or restriction of caffeine, alcohol, and salt can be implemented. In terms of medical therapy, diuretic therapy with Dyazide (triamterene and hydrochlorothiazide) can be used to decrease vestibular symptoms.5 Dietary changes and diuretics can be used for prophylaxis, while vestibulosuppressants such as valium can be used to alleviate symptoms during a Meniere’s attack. The injection of medications via the tympanic membrane into the middle ear space can also affect Meniere’s symptoms. Gentamicin, an aminoglycoside antibiotic, can be used to reduce the production of endolymph, but it has an associated risk of hearing loss.1 Intratympanic perfusion of dexamethasone contributes to the reduction of the intensity of vertigo attacks, decreases the intensity of tinnitus, and improves the average hearing threshold.6
When these more conservative therapies fail, patients can proceed to more invasive and ablative options, which include endolymphatic sac (ELS) decompression, labyrinthectomy, and vestibular neurectomy. ELS decompression offers the opportunity to preserve hearing, while labyrinthectomy and vestibular neurectomy will destroy any residual hearing in the affected ear.
Rationale for Treatment
This patient had been followed for several years for his condition and was only referred for a second opinion of management due to the inability of conservative management to continue to control his symptoms. Dietary changes and diuretic therapy had little impact. Initially he responded well to short courses of oral steroids and to several rounds of intratympanic steroid administration, but ultimately his symptoms persisted and proved debilitating.
Special Considerations
Although ELS decompression carries with it the expectation of preserved hearing due to the surgical approach, there remains a risk of hearing loss with the procedure. If the patient did not have serviceable hearing in the contralateral ear, one would likely not operate on an individual’s “only-hearing ear.”
Discussion
While hearing preservation is a key component of performing this particular approach to the vestibular system, the primary indication for surgery is ongoing episodic vertigo despite appropriate medical treatment. Although the pathophysiology was not clear at the time, the first surgical procedure to treat Meniere’s disease was performed in 1927. Portmann made a small incision to open the ELS in an attempt to decrease endolymphatic pressure.7 In 1962, a subarachnoid shunt to drain endolymphatic hydrops was described by William House.8
There are numerous reports regarding various techniques and materials used for the procedure, each describing improvements in hearing, vertigo episodes, or quality of life.9-11 In 2014, Sood et al. performed a meta-analysis regarding the current techniques and their efficacy for controlling vertigo and maintaining hearing.12 They found that both decompression alone as well as shunting into the mastoid cavity resulted in effective vertigo control for both the short term (12–24 months) and the long term (greater than 24 months) in patients who had no success with medical therapy. Even with newer techniques such as endolymphatic duct blockage, ELS surgery remains an excellent non-destructive surgical option for patients with symptoms of incapacitating endolymphatic hydrops.13
Equipment
We used a Silastic sheet (Dow Corning, Midland, Michigan, USA).
Disclosure
Author C. Scott Brown also works as editor of the Otolaryngology section of the Journal of Medical Insight.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
References
- Packer MD, Welling DB. Surgery of the endolymphatic sac. In: Brackmann D, Shelton C, Arriaga MA, eds. Otologic Surgery. 3rd ed. Philadelphia, PA: Saunders; 2010:411-428.
- Silverstein H, Smouha E, Jones R. Natural history vs. surgery for Meniere's disease. Otolaryngol Head Neck Surg. 1989;100(1):6-16. doi:10.1177/019459988910000102.
- Havia M, Kentala E, Pyykkö I. Hearing loss and tinnitus in Meniere's disease. Auris Nasus Larynx. 2002;29(2):115-119. doi:10.1016/S0385-8146(01)00142-0.
- Okuno T, Sando I. Localization, frequency, and severity of endolymphatic hydrops and the pathology of the labyrinthine membrane in Meniere's disease. Ann Otol Rhinol Laryngol. 1987;96(4):438-445. doi:10.1177/000348948709600418.
- van Deelen GW, Huizing EH. Use of a diuretic (Dyazide®) in the treatment of Ménière's disease: a double-blind cross-over placebo-controlled study. ORL J Otorhinolaryngol Relat Spec. 1986;48(5):287-292. doi:10.1159/000275884.
- Sanković-Babić S, Kosanović R, Ivanković Z, Babac S, Tatović M. [Intratympanic corticosteroid perfusion in the therapy of Meniere's disease]. Srp Arh Celok Lek. 2014;142(5-6):291-295. doi:10.2298/SARH1406291S.
- Portmann G. The saccus endolymphaticus and an operation for draining the same for the relief of vertigo. J Laryngol Otol. 1927;42(12):809-817. doi:10.1017/S0022215100031297.
- House WF. Subarachnoid shunt for drainage of endolymphatic hydrops. A preliminary report. Laryngoscope. 1962;72(6):713-729. doi:10.1288/00005537-196206000-00003.
- Durland WF Jr, Pyle GM, Connor NP. Endolymphatic sac decompression as a treatment for Meniere's disease. Laryngoscope. 2005;115(8):1454-1457. doi:10.1097/01.mlg.0000171017.41592.d0.
- Convert C, Franco-Vidal V, Bebear JP, Darrouzet V. Outcome-based assessment of endolymphatic sac decompression for Ménière's disease using the Ménière's disease outcome questionnaire: a review of 90 patients. Otol Neurotol. 2006;27(5):687-696. doi:10.1097/01.mao.0000227661.52760.f1.
- Kim SH, Ko SH, Ahn SH, Hong JM, Lee WS. Significance of the development of the inner ear third window effect after endolymphatic sac surgery in Ménière disease patients. Laryngoscope. 2012;122(8):1838-1843. doi:10.1002/lary.23332.
- Sood AJ, Lambert PR, Nguyen SA, Meyer TA. Endolymphatic sac surgery for Ménière's disease: a systematic review and meta-analysis. Otol Neurotol. 2014;35(6):1033-1045. doi:10.1097/MAO.0000000000000324.
- Garcia MLF, Segura CL, Lesser JCC, Pianese CP. Endolymphatic sac surgery for Ménière's disease – current opinion and literature review. Int Arch Otorhinolaryngol. 2017;21(2):179-183. doi:https://doi.org/10.1055/s-0037-1599276.
Cite this article
Brown CS, Cunningham III CD. Endolymphatic sac decompression. J Med Insight. 2023;2023(202). doi:10.24296/jomi/202.