
Tying Arthroscopic Knot for Glenoid Suture Anchor
Main Text
Table of Contents
Abstract
As arthroscopic and minimally-invasive procedures have become increasingly more common over the past decade, a versatile understanding of several arthroscopic knot tying techniques is essential for reproducible and reliable repairs. While there are numerous descriptions of unique arthroscopic knots, selection and correct implementation is critical for adequate soft tissue fixation and successful patient outcomes. Specifically, the Roeder knot, a type of locking sliding knot, with 3 alternating half hitches, has been described to provide the loop and knot security among other sliding knot techniques. Therefore, the Roeder knot has emerged as a preferred knot tying technique amongst orthopedic surgeons, especially in the setting of arthroscopic shoulder stabilization procedures. In this case, we describe the basic fundamentals of performing a Roeder knot with 3 alternating half hitches to anchor the labrum to the glenoid in the setting of an arthroscopic Bankart repair.
Keywords
Bankart repair; shoulder; arthroscopy; labrum; locking sliding knot.
Case Overview
Background
Anterior shoulder instability accounts for the majority of shoulder instability cases in young, active, and athletic populations,1,2 and most often occurs due to traumatic dislocation events,2,3 such as falling on an outstretched arm with an externally rotated and abducted shoulder. As the primary restraint to anteroinferior translation of the humeral head, the anteroinferior glenohumeral ligament and labrum are often compromised during these pathologic events, resulting in a Bankart lesion, which accounts for up to 90% of traumatic anterior shoulder instability cases.4 As nonoperative treatment for Bankart lesions have been reported to have 60 to 90% recurrence rates,2,5 surgical treatment has emerged as the gold standard. Specifically, arthroscopic Bankart repair has been increasingly performed, as it avoids a subscapularis split, larger incisions, and has been reported to improve postoperative range of motion when compared to open Bankart repair procedures.6,7
Focused History of Patient
A 17-year-old female softball pitcher presented to the orthopedic clinic with chronic anterior instability of the left shoulder. The patient denied acute injury and had attempted approximately 1 year of nonoperative treatment with physical therapy. However, the patient continued to have recurrent anterior instability with pain. The patient was otherwise healthy and had no history of previous injury of the left shoulder and a healthy contralateral shoulder.
Physical Exam
The patient was first evaluated for possible neurologic injury by assessing normal axillary sensation and deltoid strength. The patient had normal rotator cuff muscle strength. Physical examination findings included a positive anterior apprehension test and a positive anterior relocation test. When assessing for multidirectional instability, the patient reported no pain or feelings of instability when applying the posterior load and shift, Kim, and jerk tests and had no visual signs of a sulcus after applying an inferior load to the shoulder. These physical examination findings lead to suspicion of an anterior capsular injury.
Imaging
The patient had a thorough imaging workup including a standard radiograph series with AP, Axillary, and West Point views which did not demonstrate a Hill-Sachs lesion or glenoid bone loss. The glenohumeral joint had normal reduction without superior migration of the humeral head or an abnormal acriomiohumeral distance. MRI imaging revealed separation of the anterior labrum from the glenoid rim at the 3- to 5-o’clock position without signs of bony avulsion of the glenoid (Figure 1). The long head of the biceps tendon appeared normal without signs of a SLAP lesion, and an intact posterior labrum as suspected from negative physical examination findings. No signs of a possible concomitant HAGL lesion was detected and the rotator cuff was intact. CT scans were not necessary in this case because there was no evidence of significant glenoid bone loss of the shoulder with MRI.
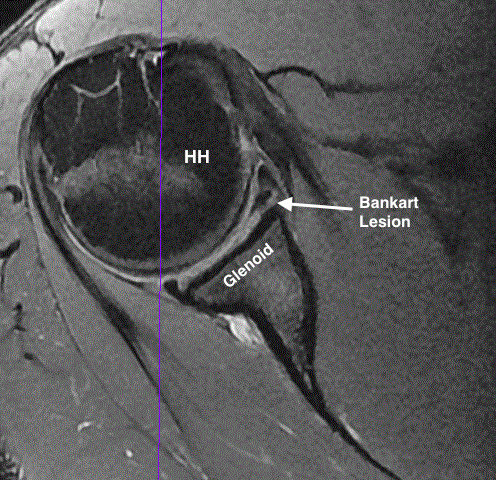
Figure 1. Axial MRI showing a Bankart lesion in a left shoulder.
Natural History
Historically, conservative treatment is typically performed with rest and immobilization of the arm with a sling in adduction and internal rotation for 3 to 6 weeks.2 Following immobilization, physical therapy is recommended, focusing on range of motion, pain control, and strengthening of the deltoid and rotator cuff muscles. However, conservative management has been reported to result in higher recurrence rate when compared to surgical treatment options,8 possibly predisposing patients to anterior glenoid bone loss over time. Other options have suggested immobilization in 30o of external rotation and has demonstrated positive results when compared to standard immobilization, although no consensus has yet been reached regarding its efficacy to reduce recurrence rates after long-term follow-up.2,9–12
Options for Treatment
Patient lifestyle should be considered for each unique case. In young, athletic populations who wish to return to normal levels of activity, surgical treatment should be considered. This is because conservative management of this patient population has been reported to result in 60 to 90% recurrence rates.2,5 Open or arthroscopic treatment can be considered, depending on concomitant injury such as a HAGL lesion, which is typically treated with open repair.13–15
Rationale for Treatment
While open repair has been suggested to have lower recurrence rates than arthroscopic repair,2 patients who undergo open repair may be susceptible to higher rates of glenohumeral joint stiffness, especially in external rotation. Therefore, less invasive arthroscopic treatment may be indicated for high-demand athletes that require high degrees of external rotation as needed in this case report.2 After discussing the risks of benefits of arthroscopic Bankart repair with the patient and addressing all questions, the patient elected to proceed with surgical treatment.
Discussion
Our preferred technique for arthroscopic Bankart repair begins with placing the patient in lateral decubitus position. Standard arthroscopic portals are made and the Bankart repair is performed through the posterolateral portal to allow adequate visualization for anchor placement and anatomic reduction of the glenoid labrum. In this case, we chose to utilize an arthroscopic knot-tying suture anchor repair. All knots were tied and passed through the anterolateral portal.
While there are numerous descriptions of unique arthroscopic knots, selection and correct implementation is critical for adequate soft tissue fixation and successful patient outcomes. Specifically, the Roeder knot, a type of locking sliding knot, with three alternating half hitches using high-strength suture (FiberWire, Arthrex Inc., Naples, FL) as described in this case has been reported to provide superior loop and knot security among other sliding knot techniques.16–18 Therefore, the biomechanical properties of the Roeder knot can provide adequate fixation of the detached capsulolabrum back to its anatomic position, and reduce the risk of knot slippage or slack in glenoid suture anchor fixation.16
Heterogenous biomechanical and clinical studies have made it difficult to reach a consensus on the optimal knot-tying technique for the Bankart repair. Although the use of the Roeder knot as a knot-tying technique for Bankart repair has not been specifically evaluated in clinical outcome studies, other sliding knot variations have been reported to provide improved patient outcomes following arthroscopic stabilization.7,19–21 However, poor outcomes may derive from placing the knot along the cartilage of the glenoid, which can result in knot arthropathy. Abrasion of the suture and knot slippage can also result in increased displacement of labrum over time.16 However, the addition of three reverse half hitches on alternating posts may reduce knot slippage and increase internal structure resistance.18,20,22–24
Knotless suture anchors are another option for arthroscopic Bankart repair and have been described to be less technically demanding.6,7 However, it has been reported that this technique may not adequately secure the glenoid labrum when compared to knot-tying techniques in biomechanical studies.25 Furthermore, late disengagement and gap formation between the labrum and glenoid rim have also been described in clinical studies. In contrast, a more recent clinical study reported similar clinical VAS and Constant scores between knotless suture anchors and the sliding hangman’s knot.7 Therefore, the choice between utilizing knotless or knot-tying arthroscopic techniques may be left up to the preference and experience of the surgeon. To provide clarity in the current literature, the authors emphasize that future randomized control studies evaluating the clinical efficacy between unique knot-tying techniques and knotless suture anchors should be performed to determine the optimal arthroscopic Bankart repair technique.
Roeder Knot-Tying Technique
- Each suture anchor is fixed using a Roeder knot with excellent tension re-approximating a large bumper placed at the 5-o’clock position.
- The post limb is always designated as the limb in the capsule and the non-post is on the glenoid. The post limb is shortened to approximately six inches.
- A Webster needle driver is clamped to the post limb.
- The non-post limb is looped under the post limb and then looped back under the non-post limb.
- The non-post limb is again looped under both the post and non-post limbs.
- Finally, the non-post limb is looped back under only the post limb and then placed down through the created triangle between the two limbs.
- As the knot is tightened locking areas are created both close to the labrum and then further away from the labrum. This allows the knot to become tighter as it is pushed down to the labrum.
- The non-post limb is then left alone, and the knot is first cinched down with a knot pusher passed the labrum to optimize the biomechanics of the knot.
- The knot can be rocked back and forth to remove the slack out of the sliding knot system.
- The knot is further secured with three half hitches with alternating posts.
- The suture is then cut with a cutter device, leaving a few millimeters of suture tail.
- Knots are repeated for each remaining suture anchor.

Figure 2. Arthroscopic Roeder Knot-Tying Technique. The post limb is depicted in blue, and the non-post limb is depicted in green. The non-post limb should be longer than the post limb; however, it is not depicted that way for better visualization of the knot.
Equipment
- 2.8-mm Bio-FASTak with FiberWire; Arthrex Inc., Naples, FL
- Spectrum suture passer (ConMed Linvatec, Largo, FL)
- Knot pusher
- Arthrex Shoulder Suspension System
Disclosures
Matthew T. Provencher has the following disclosures to report: is a paid consultant for Arthrex and the Joint Restoration Foundation (Allosource); receives intellectual property royalties from Arthrex; receives publishing royalties from SLACK Inc; is an editorial or governing board member for Arthroscopy, Knee, Orthopedics, and SLACK Inc; and is a board or committee member for AANA, AAOS, AOSSM, ASES, ISAKOS, the San Diego Shoulder Institute, and the Society of Military Orthopaedic Surgeons.
All other authors (ZSA and LAP) have no disclosures to report.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
References
- Arciero RA, Wheeler JH, Ryan JB, McBride JT. Arthroscopic Bankart repair versus nonoperative treatment for acute, initial anterior shoulder dislocations. Am J Sports Med. 1994;22(5):589-594. doi:10.1177/036354659402200504.
- Dumont GD, Russell RD, Robertson WJ. Anterior shoulder instability: a review of pathoanatomy, diagnosis and treatment. Curr Rev Musculoskelet Med. 2011;4(4):200-207. doi:10.1007/s12178-011-9092-9.
- Hovelius L, Augustini BG, Fredin H, Johansson O, Norlin R, Thorling J. Primary anterior dislocation of the shoulder in young patients. A ten-year prospective study. J Bone Joint Surg Am. 1996;78(11):1677-1684.
- Owens BD, Nelson BJ, Duffey ML, et al. Pathoanatomy of first-time, traumatic, anterior glenohumeral subluxation events. J Bone Joint Surg Am. 2010;92(7):1605-1611. doi:10.2106/JBJS.I.00851.
- Marans HJ, Angel KR, Schemitsch EH, Wedge JH. The fate of traumatic anterior dislocation of the shoulder in children. J Bone Joint Surg. 1992;74(8):1242-1244.
- Cooke SJ, Starks I, Kathuria V. The results of arthroscopic anterior stabilisation of the shoulder using the bioknotless anchor system. Sports Med Arthrosc Rehabil Ther Technol. 2009;1(1):2. doi:10.1186/1758-2555-1-2.
- Ng DZ, Kumar VP. Arthroscopic Bankart repair using knot-tying versus knotless suture anchors: is there a difference? Arthroscopy. 2014;30(4):422-427. doi:10.1016/j.arthro.2014.01.005.
- Brophy RH, Marx RG. The treatment of traumatic anterior instability of the shoulder: nonoperative and surgical treatment. Arthroscopy. 2009;25(3):298-304. doi:10.1016/j.arthro.2008.12.007.
- Itoi E, Hatakeyama Y, Sato T, et al. Immobilization in external rotation after shoulder dislocation reduces the risk of recurrence. A randomized controlled trial. J Bone Joint Surg Am. 2007;89(10):2124-2131. doi:10.2106/JBJS.F.00654.
- Tanaka Y, Okamura K, Imai T. Effectiveness of external rotation immobilization in highly active young men with traumatic primary anterior shoulder dislocation or subluxation. Orthopedics. 2010;33(9):670. doi:10.3928/01477447-20100722-07.
- Itoi E, Hatakeyama Y, Kido T, et al. A new method of immobilization after traumatic anterior dislocation of the shoulder: a preliminary study. J Shoulder Elbow Surg. 2003;12(5):413-415. doi:10.1016/S105827460300171X.
-
Finestone A, Milgrom C, Radeva-Petrova DR, et al. Bracing in external rotation for traumatic anterior dislocation of the shoulder. J Bone Joint Surg Br. 2009;91-B(7):918-921. doi:10.1302/0301-620X.91B7.22263.
- Aman ZS, Kennedy MI, Sanchez A, et al. Mini-open repair of the floating anterior inferior glenohumeral ligament: combined treatment of Bankart and humeral avulsion of the glenohumeral ligament lesions. Arthrosc Tech. 2018;7(12):e1281-e1287. doi:10.1016/j.eats.2018.08.015.
- Godin JA, Sanchez G, Kennedy NI, Ferrari MB, Provencher MT. Open repair of an anterior humeral avulsion of the glenohumeral ligament. Arthrosc Tech. 2017;6(4):e1367-e1371. doi:10.1016/j.eats.2017.05.019.
- Provencher M, McCormick F, LeClere LE, Dewing CB, Solomon DJ. A prospective outcome evaluation of humeral avulsions of the glenohumeral ligament (HAGL) tears repairs in an active population. Orthop J Sports Med. 2014;2(3 suppl). doi:10.1177/2325967114S00013.
- Longo UG, Buchmann S, Berton A, Maffulli N, Denaro V. Arthroscopic knots and strength sutures for rotator cuff repair. Sports Med Arthrosc Rev. 2011;19(3):251-265. doi:10.1097/JSA.0b013e3182199373.
- Shah MR, Strauss EJ, Kaplan K, Jazrawi L, Rosen J. Initial loop and knot security of arthroscopic knots using high-strength sutures. Arthroscopy. 2007;23(8):884-888. doi:10.1016/j.arthro.2007.02.007.
- Lo IKY, Burkhart SS, Chan KC, Athanasiou K. Arthroscopic knots: determining the optimal balance of loop security and knot security. Arthroscopy. 2004;20(5):489-502. doi:10.1016/j.arthro.2004.03.005.
- Cho NS, Lubis AMT, Ha JH, Rhee YG. Clinical results of arthroscopic bankart repair with knot-tying and knotless suture anchors. Arthroscopy. 2006;22(12):1276-1282. doi:10.1016/j.arthro.2006.07.005.
- Kim SH, Yoo JC, Wang JH, Choi KW, Bae TS, Lee CY. Arthroscopic sliding knot: how many additional half-hitches are really needed? Arthroscopy. 2005;21(4):405-411. doi:10.1016/j.arthro.2004.12.010.
- Gartsman GM, Roddey TS, Hammerman SM. Arthroscopic treatment of anterior-inferior glenohumeral instability: two to five-year follow-up. J Bone Joint Surg Am. 2000;82(7):991-1003.
- Ilahi OA, Younas SA, Alexander J, Noble PC. Cyclic testing of arthroscopic knot security. Arthroscopy. 2004;20(1):62-68. doi:10.1016/j.arthro.2003.11.002.
- Jo CH, Lee JH, Kang SB, et al. Optimal configuration of arthroscopic sliding knots backed up with multiple half-hitches. Knee Surg Sports Traumatol Arthrosc. 2008;16(8):787-793. doi:10.1007/s00167-008-0497-y.
- Lee TQ, Matsuura PA, Fogolin RP, Lin AC, Kim D, McMahon PJ. Arthroscopic suture tying: a comparison of knot types and suture materials. Arthroscopy. 2001;17(4):348-352. doi:10.1053/jars.2001.23227.
- Zumstein M, Jacob HAC, Schneeberger AG. In vitro comparison of standard and knotless metal suture anchors. Arthroscopy. 2004;20(5):517-520. doi:10.1016/j.arthro.2004.03.007.
Cite this article
Aman ZS, Peebles LA, Provencher MT. Tying arthroscopic knot for glenoid suture anchor. J Med Insight. 2024;2024(f3). doi:10.24296/jomi/f3.
