Laparoscopic Sigmoid Resection for Diverticulitis
Main Text
Table of Contents
Abstract
Laparoscopic sigmoid resection is indicated for disease of the distal sigmoid or rectum that requires resection, most notably diverticulitis and colorectal cancer. Here, we perform an sigmoid resection for diverticular disease. In this procedure, we used four laparoscopic port sites. In the first step, we mobilized the splenic flexure and left colon to allow for a tension-free colorectal anastomosis low in the pelvis. Second, the mesorectum was dissected to mobilize the rectum down to the level of the pelvic floor. Third, the left colic and inferior mesenteric arteries were ligated, the colonic mesentery was transected with an energy device, and the distal resection margin was stapled intracorporeally. Fourth, the specimen was extracorporealized through the umbilical port site, and the proximal transection was performed. Finally, an anvil was inserted, and the colon was placed back into the abdomen where a trans-anal, stapled end-to-side Baker-type anastomosis was performed and endoscopically tested for leaks.
Case Overview
Background
Diverticulosis is a process by which colonic mucosa and submucosa herniate between muscular layers of the bowel wall to form false diverticula. Diverticulosis occurs in 60% of Americans aged greater than 60 years; it is thought to be associated with a low fiber, a western diet, obesity, and physical inactivity.1 Although diverticulosis can occur anywhere in the colon, it presents more commonly in the distal left colon and sigmoid. Diverticula can become obstructed with fecal matter, resulting in venous congestion, tissue ischemia, inflammation, infection, and in severe cases, perforation, a process referred to as diverticulitis.2 Diverticulitis affects 10–25% of patients with diverticulosis, and represents a significant healthcare burden in the United States, accounting for 2.7 million outpatient visits and over 200,000 inpatient admissions each year.3 Diverticulitis presents with varying degrees of severity. Uncomplicated disease is limited to local inflammation and pain, whereas complicated diverticulitis is associated with perforation that can result in abscess, phlegmon, or purulent/feculent peritonitis that may require urgent surgical intervention. Long-term complications of diverticulitis include stricture and fistula formation to surrounding structures.
Treatment for diverticulitis depends on disease severity and acuity. Uncomplicated disease is initially treated with antibiotics, intravenous fluids, and bowel rest. Complicated disease may require surgical intervention. For perforated diverticulitis with abscess, percutaneous drainage may be indicated for source control. Purulent or feculent peritonitis may require urgent surgical intervention, usually with resection of the diseased colon, and either fecal diversion with end-colostomy (Hartmann’s procedure) or primary colorectal anastomosis if conditions permit.4 There are certain indications for colectomy on an elective basis for diverticulitis. Surgery is recommended for patients who are at high risk for infection, e.g. immunosuppressed transplant patients, patients with prior episodes of diverticulitis with abscess that required drainage, those with long-term complications such as fistula or stricture, and for patients who have had multiple recurrent episodes and would like to prevent future occurrences.5
In the present case, we perform a laparoscopic sigmoid resection for sigmoid diverticulitis in a 70-year-old patient who had three prior episodes of uncomplicated diverticulitis over the prior year. In this procedure, the sigmoid and proximal rectum were excised, and a colorectal anastomosis was performed. The procedure adequately resected the diseased portion of colon, effectively treating this condition.
Focused History of the Patient
The patient is a 70-year-old female presenting with recurrent, uncomplicated diverticulitis that was negatively impacting her quality of life. She had experienced 12–15 episodes over the prior decade, three of which occurred within the last 12 months, and she presented for elective resection. The prior episodes were treated with antibiotics. Her other medical history is notable for early stage breast cancer treated with lumpectomy. She had a surgical history notable for a salpingectomy and oophorectomy to treat an ectopic pregnancy over 30 years prior. She had an American Society of Anaesthesiologist score of 2, and her body mass index was 21. Preoperative evaluation included a colonoscopy that confirmed diverticulosis without evidence of malignancy.
Physical Exam
The patient had an unremarkable physical exam. In the office, she was in no apparent distress with normal vital signs. She had a normal habitus. Her abdominal exam was significant for prior surgical scars, no evidence of hernias, and no tenderness to palpation.
Imaging
The patient’s most recent episode of diverticulitis was 10 weeks prior to her elective surgery. At that time, she presented to the emergency department with abdominal pain and underwent a computed tomography (CT) scan of the abdomen and pelvis with oral and intravenous contrast, revealing evidence of sigmoid diverticulitis without perforation (Figure 1).
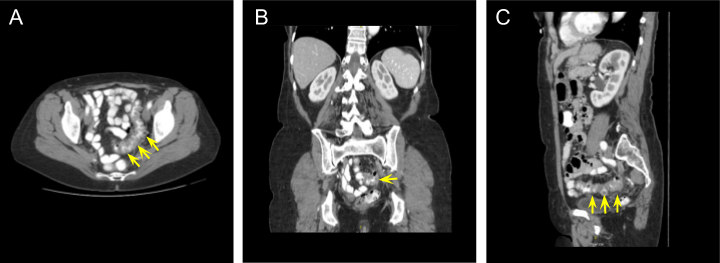
Figure 1. Abdominal and Pelvic CT Scan. CT scan of the abdomen and pelvis with intravenous and oral contrast revealing evidence of uncomplicated sigmoid diverticulitis. The diseased tissue is shown in (A) axial, (B) coronal, and (C) sagittal views. Yellow arrows point to the diseased segment of colon.
Natural History
Our understanding of the natural history of diverticulitis has recently come under scrutiny. It was previously thought that diverticulitis is a progressive condition in which recurrent disease is associated with more severe complications. This paradigm was the foundation for an aggressive surgical approach. However, more recent data suggested that complications are most likely to occur during the first episode, with decreased severity during subsequent episodes.6 In response to this information, a more conservative approach to treatment is currently practiced. Nevertheless, the risk of recurrence does increase with subsequent episodes. The risk of recurrence after a first episode of uncomplicated diverticulitis is approximately 20% at 10 years, increasing to greater than 50% after a second episode.7
Options for Treatment
The only potentially curative therapy for diverticulitis remains surgical resection of the diseased tissue. Nevertheless, elective colectomy is not essential, and the patient should discuss the risks and benefits of an operation with their surgeon. Other potential treatments, including dietary changes, probiotics, and certain pharmacologic agents are under investigation; however, there is currently insufficient evidence to support these therapies in consensus guidelines.
Rationale for Treatment
The rationale for therapy is context-dependent. For acute disease, the goal of treatment is to control infection and associated inflammation. This has typically been accomplished with bowel rest and antibiotics for uncomplicated disease. In certain non-severe, uncomplicated cases, diverticulitis can be self-limiting and requires no medical therapy.8 For perforated disease, source control of infection and sepsis management, when relevant, are the primary goals. Source control may include percutaneous drainage for abscess, and for purulent or feculent spillage, colectomy with abdominal washout may be necessary.
For chronic disease, management is on an elective basis. The rationale for surgical intervention is predicated on achieving one of three goals, depending on the clinical scenario: (1) prevention of future recurrences in a high-risk patient or someone with multiple prior episodes; (2) treatment of long-term complications such as fistula or stricture; or (3) definitive therapy for refractory disease that has been unresponsive to medical management. Ultimately, the goal of surgical excision is to cure the patient of diverticular disease.
Special Considerations
There are three types of patients that are likely to most benefit from surgical excision for diverticular disease: First, patients that are immunocompromised or have significant medical comorbidities. These patients are at higher risk of serious complications from diverticular infection in the event of a recurrence; second, patients who have experienced multiple recurrences of diverticulitis and are therefore at increased risk of future episodes; third, patients who previously experienced complicated diverticulitis with an abscess that required percutaneous drainage. These patients are at increased risk for recurrent complicated disease, potentially resulting in significant morbidity or mortality. Finally, contraindications to surgery are generally limited to individuals with significant medical comorbidities, e.g. cardiopulmonary disease, that precludes them from undergoing general anesthesia.
Discussion
As we have shown in this video, the main procedural steps for this operation are as follows: (1) mobilize the descending colon in a lateral to medial fashion; (2) mobilize the transverse colon and splenic flexure by taking down the gastrocolic attachments; (3) take down the peritoneal reflection and mobilize the rectum; (4) ligate the inferior mesenteric artery (IMA) and left colic artery; (5) transect the rectum with an Endo GIA stapler and extracorporealize the colon to perform the proximal transection; and (6) perform an EEA colorectal anastomosis with endoscopic leak test. This approach to the sigmoid resection results in extensive mobilization of the proximal colon, allowing for a large resection with subsequent tension-free anastomosis deep in the pelvis. The blood supply for the colonic conduit is dependent on the marginal artery of Drummond, which cannot be damaged during the operation.
Surgical approaches to rectosigmoid dissection have undergone significant evolution. The first published reports on rectal mobilization and resection date back to the early 1800s and involved perineal and trans-sacral approaches with high morbidity.9 The low anterior approach was described by Hartmann in 1921, and subsequent modifications for improved technique were published throughout the early 1900s. In the modern era, two main technological advancements have fundamentally changed and improved our approach to surgery of the colon and rectum. First, the development of trans-anal, circular stapling devices has allowed for efficient and effective stapled anastomoses low in the pelvis. Second, the advent of laparoscopy in the 1980s allowed for minimally invasive colorectal surgery with excellent visualization of the pelvis during the mesorectal dissection. As a result, the majority of elective sigmoid and rectal operations can be performed laparoscopically through several small anterior port sites with low morbidity and mortality and faster recovery.
The recommendation to perform elective rectosigmoid colectomy on a patient with recurrent uncomplicated diverticulitis should be individualized. After a single episode of uncomplicated disease, the risk of recurrence ranges from 12–23% with less than 6% risk of recurrent complicated disease.10 In these cases, the potential risk for complications from surgery must be balanced with the projected risk of future disease, with consideration of immune function and comorbidities. For patients with complicated disease on the first episode or multiple prior recurrences, the current recommendations are to offer an elective colon resection after resolution of the most recent episode, given the increased risk of recurrence.11 After surgical resection for sigmoid diverticulitis, there is an approximately 15% chance of recurrence with a 10–20% risk of postoperative complications.3
There are several active areas of investigation that may improve our understanding and treatment of diverticulitis going forward. These areas include the gut microbiome, genetic factors, diet and lifestyle, and chronic inflammatory signaling. More effective medical therapies might help to improve surgical outcomes by reducing disease severity, thereby mitigating adverse operative conditions at the time of surgery.
Patient Outcome Statistics from the Procedure
- Operative time: 90 minutes
- Estimated blood loss: 50 mL
- Fluids: 1200 mL crystalloid
- Length of Stay: Discharged from hospital to home without services on postoperative day 2
- Morbidity: no complications
- Final pathology: sigmoid diverticulitis
Equipment
- Veress needle
- Laparoscopic ports: 12 mm x2, 5 mm x2
- Laparoscope: 10-mm 30 degree
- Covidien laparoscopic harmonic scalpel
- Endo GIA™ 30-mm Reload with Tri-Staple™ Technology
- Covidien end-to-end anastomotic (EEA) stapler
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
Acknowledgments
We would like to thank Theresa Kim, MD for assisting in this operation.
References
- Peery AF, Dellon ES, Lund J, et al. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology. 2012;143:1179-87 e3. doi:10.1053/j.gastro.2012.08.002.
- Painter NS, Burkitt DP. Diverticular disease of the colon: a deficiency disease of Western civilization. Br Med J. 1971;2:450-4. doi:10.1136/bmj.2.5759.450.
- Strate LL, Morris AM. Epidemiology, pathophysiology, and treatment of diverticulitis. Gastroenterology. 2019;156:1282-98 e1. doi:10.1053/j.gastro.2018.12.033.
- Oberkofler CE, Rickenbacher A, Raptis DA. A multicenter randomized clinical trial of primary anastomosis or Hartmann's procedure for perforated left colonic diverticulitis with purulent or fecal peritonitis. Ann Surg. 2012;256:819-26; discussion 26-7. doi:10.1097/SLA.0b013e31827324ba.
- Regenbogen SE, Hardiman KM, Hendren S, Morris AM. Surgery for diverticulitis in the 21st century: a systematic review. JAMA Surg. 2014;149:292-303. doi:10.1001/jamasurg.2013.5477.
- Ritz JP, Lehmann KS, Frericks B, Stroux A, Buhr HJ, Holmer C. Outcome of patients with acute sigmoid diverticulitis: multivariate analysis of risk factors for free perforation. Surgery. 2011;149:606-13. doi:10.1016/j.surg.2010.10.005.
- Bharucha AE, Parthasarathy G, Ditah I, et al. Temporal trends in the incidence and natural history of diverticulitis: a population-based study. Am J Gastroenterol. 2015;110:1589-96. doi:10.1038/ajg.2015.302.
- Stollman N, Smalley W, Hirano I, Committee AGAICG. American Gastroenterological Association Institute Guideline on the management of acute diverticulitis. Gastroenterology. 2015;149:1944-9. doi:10.1053/j.gastro.2015.10.003.
- Inoue Y, Kusunoki M. Resection of rectal cancer: a historical review. Surg Today. 2010;40:501-6. doi:10.1007/s00595-009-4153-z.
- Hall JF, Roberts PL, Ricciardi R, et al. Long-term follow-up after an initial episode of diverticulitis: what are the predictors of recurrence? Dis Colon Rectum. 2011;54:283-8. doi:10.1007/DCR.0b013e3182028576.
- Feingold D, Steele SR, Lee S, et al. Practice parameters for the treatment of sigmoid diverticulitis. Dis Colon Rectum. 2014;57:284-94. doi:10.1097/DCR.0000000000000075.
Cite this article
Erstad DJ, Berger D. Laparoscopic sigmoid resection for diverticulitis. J Med Insight. 2023;2023(87). doi:10.24296/jomi/87.