
Descriptions of Clinical and Surgical Procedures Full Text
Cataract Extraction with Phacoemulsification and Posterior Chamber Intraocular Lens
Main Text
Table of Contents
Abstract
Cataract is a leading cause of treatable blindness in the world. While there is a significant difference in access to surgical care in developing vs. industrial nations, cataract is a significant contributor to visual impairment in both. The diagnosis of cataract is made through assessment of visual acuity, visual disability, and slit lamp biomicroscopy. Common indications for surgery include difficulty with glare, night driving, decrease in best corrected vision impairing distance and/or near vision, and impairment of view to the retina that is precluding necessary treatment. In the US, the standard for cataract extraction has become phacoemulsification. The article demonstrates and reviews the technique of cataract extraction using phacoemulsification with intraocular lens implantation using the divide-and-conquer technique.
Case Overview
Focused history
Patients with visually significant cataract will report some kind of visual decline or functional decline due to a loss of visual acuity. This can be as simple as a decline in best corrected visual acuity at distance and/or near, or it can be a more subtle loss of function, such as requiring more light for reading, difficulty with night driving, increasing glare with oncoming headlights, or solar glare when driving when the sun is low on the horizon. The critical information here lies with documenting a decrease or loss of daily functioning. This is the indication for surgical intervention.
Exam
Visual acuity
- Check patient's visual acuity with current correction.
- Pinhole can give a quick reference on whether or not refraction may be beneficial.
- Manifest refraction to achieve best corrected visual acuity.
Glare testing
- Brightness acuity test (BAT) is used to demonstrate glare.
- This test is useful for documenting visual impairment with glare in patients that have good best corrected visual acuity.
Potential acuity meter (PAM)
- This is a useful test in patients with comorbid ocular disease to help counsel the patients regarding the potential vision outcome postoperatively.
Slit lamp findings
- Lids and adnexa should be examined for any signs of blepharitis, which should be treated preoperatively. This will also give clues to any anatomic issues that may affect surgical exposure.
- Conjunctiva should be evaluated. This may affect the position of the corneal incision as there may be postsurgical changes from glaucoma surgery, or pterygium that may limit access to the corneal limbus.
- Cornea exam should focus on evidence of previous corneal surgery (refractive surgery or transplant procedures). Look for any scars or opacities from surgery, trauma, or infection that may impair the surgical view. Also, look for any signs of dystrophies that can affect the refractive outcome as well as predispose to endothelial decompensation postoperatively.
- Anterior chamber depth can give you a sense of how much space you will have to work. Short eyes with shallow chambers will have phacoemulsification done slightly more posteriorly in order to limit endothelial damage.
- Iris should be assessed for pupil dilation, transillumination defects, and pseudoexfoliation material. These are important for the assessment of surgical exposure as well as potential loss of stability of the capsular lens complex. Noting any signs of trauma, zonular compromise, and/or poor dilation will help in surgical planning. Surgeon may decide to have specialty devices available to facilitate surgery including iris hooks, Malyugin rings, capsular hooks, and capsular tension rings and segments.
- Lens should be assessed for lens opacity. The capsule and zonular support should also be assessed. Look for centration of the crystalline lens. Assess the stability of the lens. Focus should be on any sign of capsular violation or compromise. This could be congenital, traumatic, or iatrogenic. This is true also for zonular loss. Presence of any of these factors can affect the surgical approach. In patients with significant disruption, pars plana lensectomy may be the safest approach.
- Dilated exam should be performed. This will help facilitate the evaluation of the lens. Also important is the evaluation of the retina and optic nerve. This will help determine if there are other diseases that are affecting the vision, and whether cataract surgery would be beneficial or if other treatment may be needed.
Imaging studies
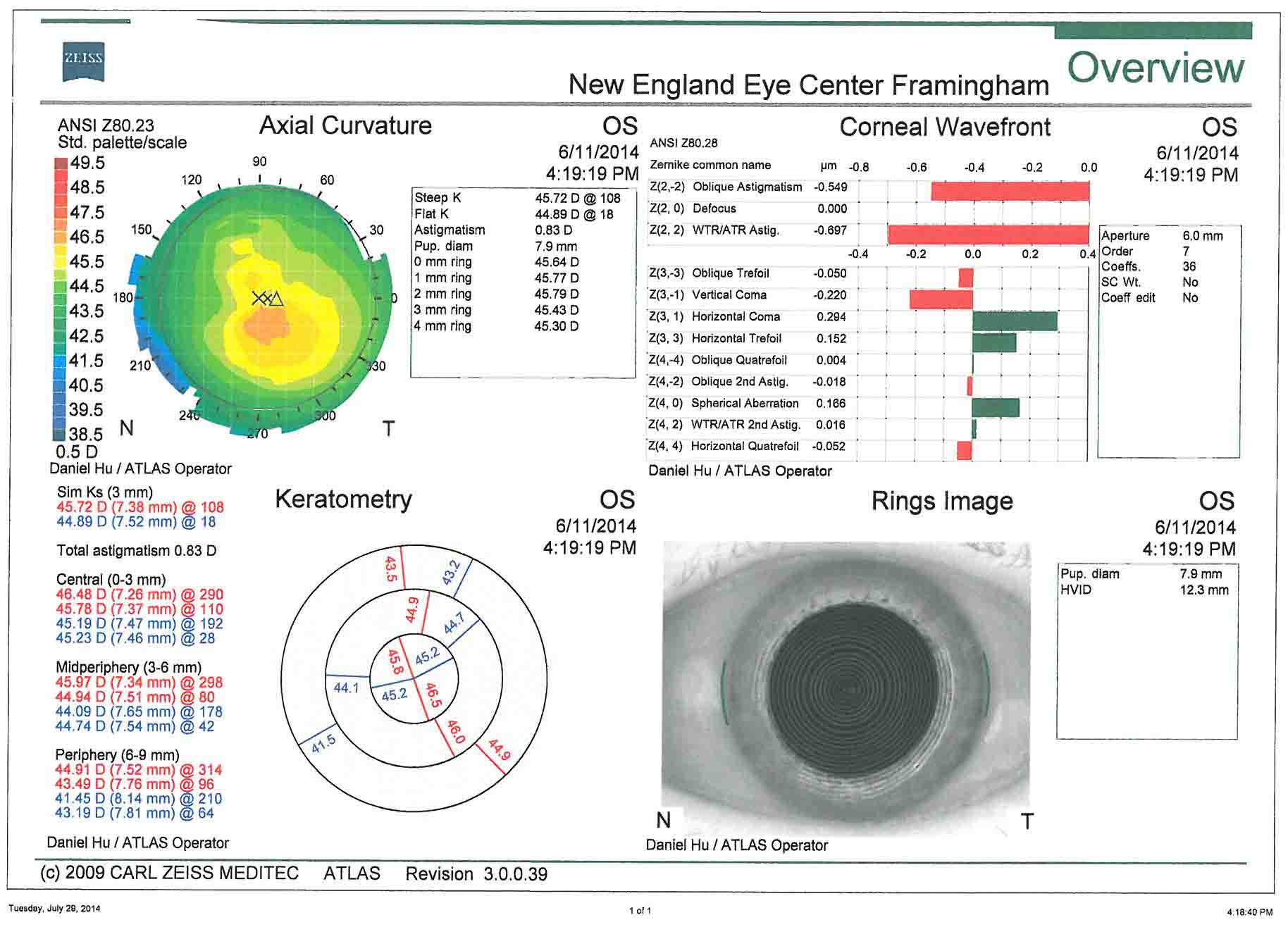
- Corneal topography- This is useful for the assessment of preoperative corneal astigmatism. Surgical planning of astigmatism management is based off of these images.
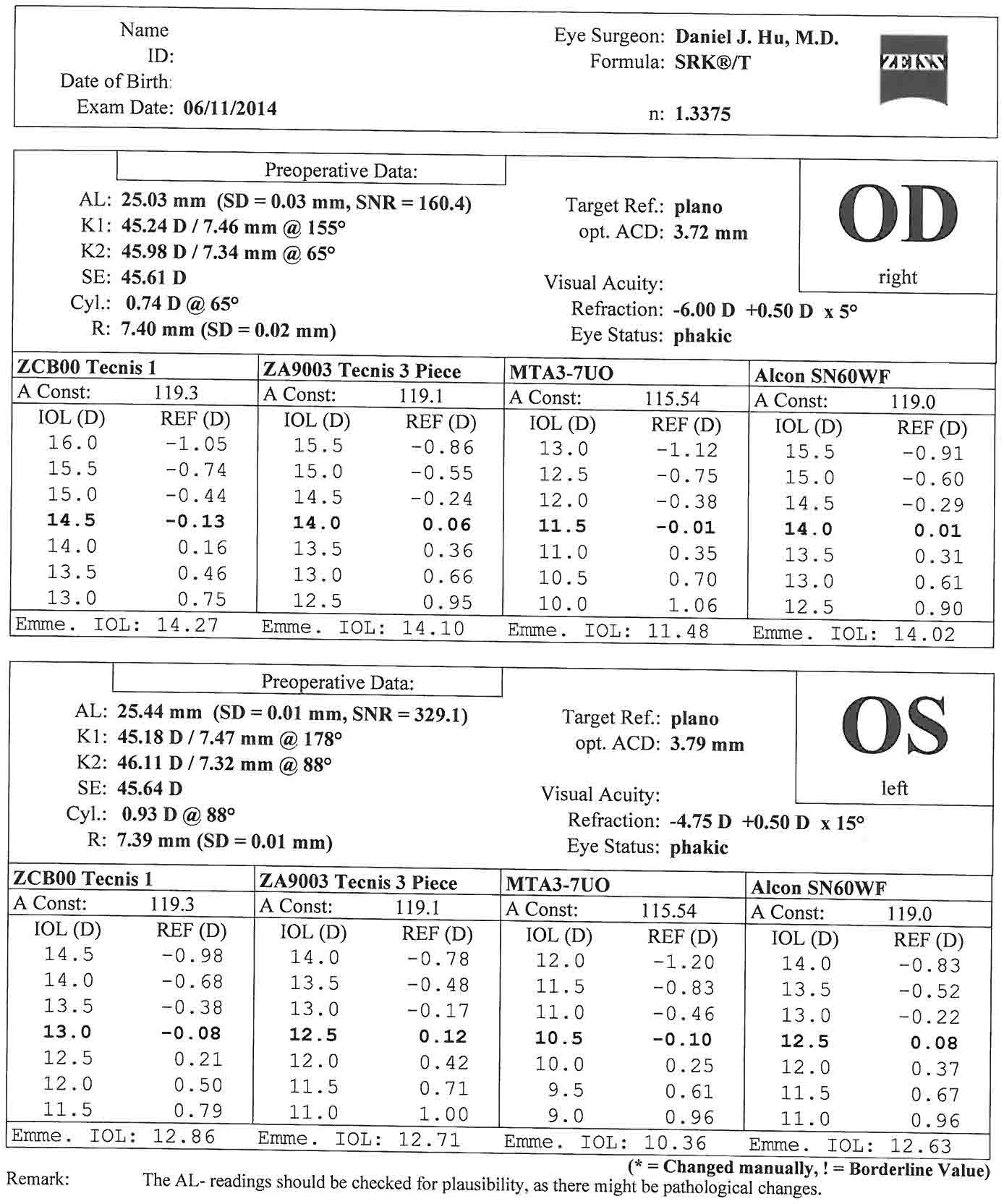
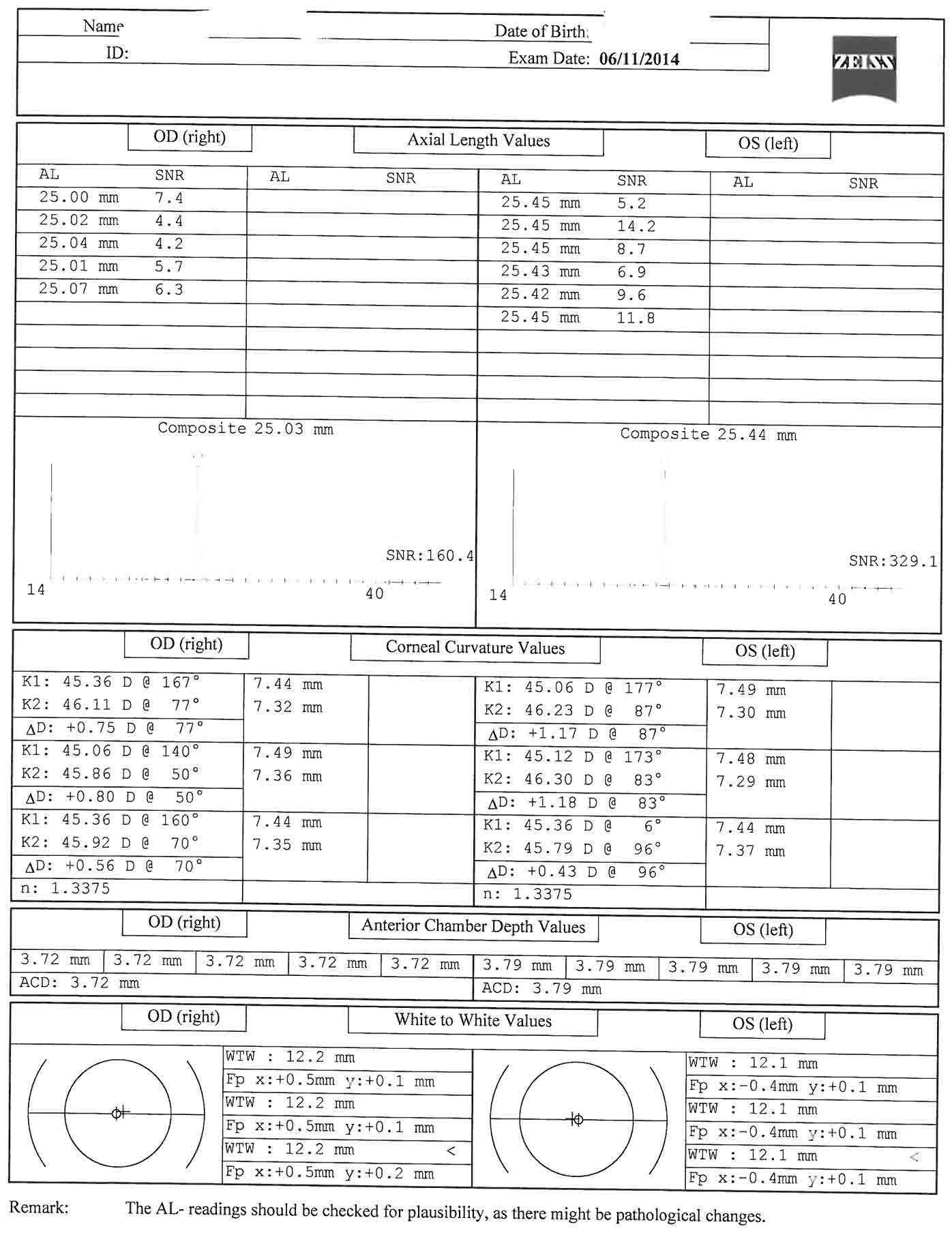
- Biometry (IOL master)- Keratometry, anterior chamber depth, white-to-white, and axial length are measured, and intraocular lens powers calculated.
- B-scan- In cases of mature cataract that impairs the view to the retina. This allows a gross assessment of retinal anatomy. Is there a retinal detachment or mass present?
- Specular microscopy- Can be performed in cases of endothelial dysfunction to assess endothelium prior to surgery.
In this case, there is less than 1 diopter of oblique corneal astigmatism in both eyes. This corroborates well with the keratometry from the biometry. In this case, corneal relaxing incisions could be used to manage the astigmatism. The patient has elected to forgo astigmatism treatment.
Natural history
- If left untreated, cataract will lead to progressive vision loss and blindness.
Options for treatment
- If the cataract is visually significant, there are limited options for treatment. Surgical intervention is necessary in order to restore vision.
Rationale for treatment in this case
- Phacoemulsification using divide-and-conquer has the advantage of being a universal technique that can be used for all degrees and types of cataract.
- Special consideration should be taken in cases of dense, mature nuclear sclerosis, zonulopathy, subluxation of the crystalline lens, or any cases with a limited view of the anterior segment.
Corneal Topography Charts

Potential Postoperative Complications
Potential postoperative complications include the following conditions:
- Corneal edema
- Descemet's membrane detachment
- Induced astigmatism
- Corneal wound burn
- Wound leak
- Epithelial downgrowth
- Toxic anterior segment syndrome (TASS)
- Intraoperative floppy iris syndrome (IFIS)
- Iridodialysis
- Cyclodialysis
- Urrets-Zavalia syndrome
- Elevated intraocular pressure
- Malignant glaucoma
- Retained lens material
- Capsular rupture
- Vitreous prolapse
- IOL complications (decentration and dislocation, pupillary capture, capsular block syndrome, uveitis-glaucoma-hyphema syndrome, pseudophakic bullous keratopathy, incorrect IOL power, IOL glare, IOL opacification)
- Anterior capsular fibrosis and phimosis
- Posterior capsular opacification
- Hemorrhage (retrobulbar hemorrhage-complication for retrobulbar anesthesia, suprachoroidal effusion, expulsive suprachoroidal hemorrhage, hyphema)
- Chronic postoperative uveitis
- Endophthalmitis
- Cystoid macular edema
- Retinal light toxicity
- Macular infarction
- Retinal detachment
Discussion
Cataract surgery has undergone considerable advancement over the last several decades that has improved the safety and efficacy of the procedure. This has been driven by a progressive movement toward decreasing surgical trauma to the eye. Modern cataract surgery has progressed from large incision techniques, such as intracapsular cataract extraction, to extracapsular cataract extraction, to now small incision phacoemulsification.1 Cataract surgery has become an exceptionally safe and successful surgical procedure. Multiple large studies have shown best corrected postoperative visual acuity of 20/40 or better in 85.5–89% of all patients, and 94.7–96% of patients without preoperative ocular comorbidities. 95% of patients were satisfied with the outcome of their surgery.2-4 However, there continue to be challenges regarding the reproducibility of the capsulotomy, the use of ultrasound and its effects on the corneal endothelium, as well as capsular complications. As the risk of significant intraoperative complications has been reduced, the expectation for visual outcomes has continued to increase. Cataract surgery and refractive surgery are increasingly linked as outcomes are being driven by the expectation of emmetropia.
Cataract surgery continues to evolve away from manual surgery to technology driven techniques. A major leap forward was the advent of phacoemulsification by Charles Kelman, MD in the 1960s. By the 1990s, phacoemulsification had become the standard for cataract surgery in developed countries. Refinements in phacoemulsification have continued to improve outcomes and decrease complications. Femtosecond laser-assisted cataract surgery is the newest technology to be incorporated into use with cataract surgery. The potential benefits of femtosecond laser-assisted cataract surgery include reproducible capsulotomy, reduction in ultrasound time, and reproducible corneal incisions. A significant reduction in ultrasound time has been shown. Femtosecond lasers have also been shown to have improved accuracy and reproducibility of capsulotomy and corneal incisions. The reproducibility of the corneal incisions is especially valuable in the context of astigmatism control.5-8 The intended benefits of these characteristics is to improve patient recovery time, reduce complications, and help achieve better refractive outcomes.
As cataract techniques have improved, so has the expectation for rapid postoperative recovery, as well as immediate refractive outcomes. Improved biometry has increased the predictability of postcataract surgery outcomes. Intraoperative aberrometry has been a tremendous asset in helping with the accuracy of IOL selection, especially in eyes with previous keratorefractive surgery.9 This predictability is critical when considering the refractive expectations of both postrefractive surgery cataract patients, and combined refractive-cataract surgery patients who are expecting immediate outcomes.
The emmetropic eye with adaptation for presbyopia has become the goal of many patients. While there is still room for this technology to mature, current technology is able to achieve this for many patients. Astigmatism can be managed at the time of surgery with on axis surgery, corneal relaxing incisions, or toric intraocular lenses.10-13 Presbyopia can be managed with monovision, multifocal, or accommodating IOLs.14-15 These advanced intraocular lenses have given patients the ability to function with greater freedom from the use of spectacle correction for the majority of their daily tasks. Advances in IOL technology will continue to drive the desire for spectacle independence postoperatively.
Equipment
- Corneal topographer- Zeiss Atlas 9000
- Biometry- Zeiss IOL Master
- Phacoemulsifier- Alcon Infiniti Vision System
- Settings
- Sculpt: Irrigation: 95 cm, Torsional: 100 (Linear), Vacuum: 90 mmHg (Linear), Aspiration: 22 cc/min (Fixed)
- Quadrant: Irrigation: 100 cm, Torsional: 100 (Linear), Vacuum: 350 mmHg (Fixed), Aspiration: 40 cc/min (Linear)
- Epinucleus: Irrigation: 95 cm, Torsional: 95 (Linear), Vacuum: 300 mmHg (Linear), Aspiration 30 cc/min (Linear)
- Cortex: Irrigation: 100 cm, Vacuum 500 mmHg (Linear), Aspiration: 35 cc/min (Linear)
- Polish: Irrigation: 95 cm, Vacuum 10 mmHg (Linear), Aspiration: 6 cc/min (Linear)
- Viscoelastic: Irrigation: 95 cm, Vacuum 600 mmHg (Linear), Aspiration: 40 cc/min (Fixed)
- Surgical microscope- Leica
- Intraocular lens- AMO Tecnis ZCB00 Intraocular lens
Disclosures
The author has no financial relationships with any of the products or equipment mentioned in this article.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
References
- Stein JD. Serious adverse events after cataract surgery. Curr Opin Ophthalmol. 2012;23(3):219-225. doi:10.1097/ICU.0b013e3283524068.
- Lundström M, Barry P, Leite E, Stenevi U. 1998 European cataract outcome study: report from the European Cataract Outcome Study Group. J Cataract Refract Surg. 2001;27(8):1176-1184. doi:10.1016/S0886-3350(01)00772-6.
- Lum F, Schein O, Schachat AP, Abbott RL, Hoskins HD Jr, Steinberg EP. Initial two years of experience with the AAO National Eyecare Outcomes Network (NEON) cataract surgery database. Ophthalmology. 2000;107(4):691-697. doi:10.1016/S0161-6420(99)00184-0.
- Jaycock P, Johnston RL, Taylor H, et al. The Cataract National Dataset electronic multi-centre audit of 55,567 operations: updating benchmark standards of care in the United Kingdom and internationally. Eye (Lond). 2009;23(1):38-49. doi:10.1038/sj.eye.6703015.
- Reddy KP, Kandulla J, Auffarth GU. Effectiveness and safety of femtosecond laser-assisted lens fragmentation and anterior capsulotomy versus the manual technique in cataract surgery. J Cataract Refract Surg. 2013;39(9):1297-1306. doi:10.1016/j.jcrs.2013.05.035.
- Abell RG, Kerr NM, Vote BJ. Toward zero effective phacoemulsification time using femtosecond laser pretreatment. Ophthalmology. 2013;120(5):942-948. doi:10.1016/j.ophtha.2012.11.045.
- Hatch KM, Talamo JT. Laser-assisted cataract surgery: benefits and barriers. Curr Opin Ophthalmol. 2014;25(1):54-61. doi:10.1097/ICU.0000000000000013.
- Roberts TV, Lawless M, Chan CCK, et al. Femtosecond laser cataract surgery: technology and clinical practice. Clin Exp Ophthalmol. 2013;41(2):180-186. doi:10.1111/j.1442-9071.2012.02851.x.
- Ianchulev T, Hoffer KJ, Yoo SH, et al. Intraoperative refractive biometry for predicting intraocular lens power calculation after prior myopic refractive surgery. Ophthalmology. 2014;121(1):56-60. doi:10.1016/j.ophtha.2013.08.041.
- Wang L, Misra M, Koch DD. Peripheral corneal relaxing incisions combined with cataract surgery. J Cataract Refract Surg. 2003;29(4):712-722. doi:10.1016/S0886-3350(02)01838-2.
- Kaufmann C, Peter J, Ooi K, et al. Limbal relaxing incisions versus on-axis incisions to reduce corneal astigmatism at the time of cataract surgery. J Cataract Refract Surg. 2005;31(12):2261-2265. doi:10.1016/j.jcrs.2005.08.046.
- Sheppard AL, Wolffsohn JS, Bhatt U, et al. Clinical outcomes after implantation of a new hydrophobic acrylic toric IOL during routine cataract surgery. J Cataract Refract Surg. 2013;39(1):41-47. doi:10.1016/j.jcrs.2012.08.055.
- Visser N, Bauer NJC, Nuijts RMMA. Toric intraocular lenses: historical overview, patient selection, IOL calculation, surgical techniques, clinical outcomes, and complications. J Cataract Refract Surg. 2013;39(4):624-637. doi:10.1016/j.jcrs.2013.02.020.
- Schmickler S, Bautista CP, Goes F, Shah S, Wolffsohn JS. Clinical evaluation of a multifocal aspheric diffractive intraocular lens. Br J Ophthalmol. 2013;97(12):1560-1564. doi:10.1136/bjophthalmol-2013-304010.
- Cumming JS, Colvard DM, Dell SJ, et al. Clinical evaluation of the Crystalens AT-45 accommodating intraocular lens: results of the U.S. Food and Drug Administration clinical trial. J Cataract Refract Surg. 2006;32(5):812-825. doi:10.1016/j.jcrs.2006.02.007.
- Gimbel HV. Divide and conquer nucleofractis phacoemulsification: development and variations. J Cataract Refract Surg. 1991;17(3):281-291. doi:10.1016/S0886-3350(13)80824-3.
Cite this article
Hu DJ. Cataract extraction with phacoemulsification and posterior chamber intraocular lens. J Med Insight. 2023;2023(7). doi:10.24296/jomi/7.
