
Arthroscopic Bankart Repair for Anterior Shoulder Instability Using a Posterolateral Portal
Main Text
Table of Contents
Abstract
A successful surgical outcome for patients with shoulder instability requires a complete preoperative evaluation, a thorough diagnostic arthroscopy to evaluate for concomitant co-pathology, and an effective postoperative therapy program tailored to the repair strategy. In addition to the Bankart lesion, the surgeon must be aware of other co-pathologies such as the HAGL lesion, the ALPSA lesion and SLAP tears, all of which may occur in concert with capsular pathology and which present as potential barriers to a successful outcome. We have previously described the use of a posterolateral arthroscopic portal, 4 cm lateral to the posterolateral corner of the acromion. This portal simplifies and improves anchor placement, trajectory, and anatomic capsulolabral repair of the inferior glenoid. In this case, we perform a hybrid repair using the posterolateral portal to place the first suture anchor at the 6 o’clock position on the glenoid and the mid-glenoid portal to place two labral tape knotless anchors.
Case Overview
Focused history
Obtain a history which includes past injury, trauma, and/or repetitive motions.- Has the patient dislocated? If so, how many times? What was the mechanism? How strong was the force required to dislocate?
- What limitations in activity have occurred? Is pain or instability present at rest? Does it interfere with sleep?
- What prior treatments, if any, has the patient already tried (i.e. physical therapy, rest, anti-inflammatory medication) and to what degree did these help?
Physical exam
- Palpate the shoulder for tenderness and document range of motion compared to the contralateral extremity. Differences between active and passive motion may indicate pain or capsular contracture.
- Test for impingement to determine whether rotator cuff tendinitis is present. If weakness is present during strength testing, it may be from deconditioning or from underlying rotator cuff or deltoid pathology.
- Tests for anterior instability
- Apprehension sign - performed with patient supine and the arm forward flexed 90 degrees and the elbow flexed 90 degrees. The patient exhibits apprehension when an anterior force is applied to the shoulder
- Relocation sign - the patient’s apprehension decreases when a posterior, supporting force is applied to the shoulder
- Sulcus sign - an inferior force is applied to the shoulder with the patient standing, arm at their side. Appearance of a depression below the acromion indicates a positive sulcus sign
Imaging
Evaluation should begin with a complete trauma series of the shoulder including a true AP, scapular Y and axillary views. A West Point view can be helpful in evaluating glenoid bone loss and Stryker view is best for seeing a Hill-Sachs lesion, if present.MRI is the modality of choice for evaluating the presence and extent of a labral tear. Intra-articular contrast will increase the sensitivity and specificity.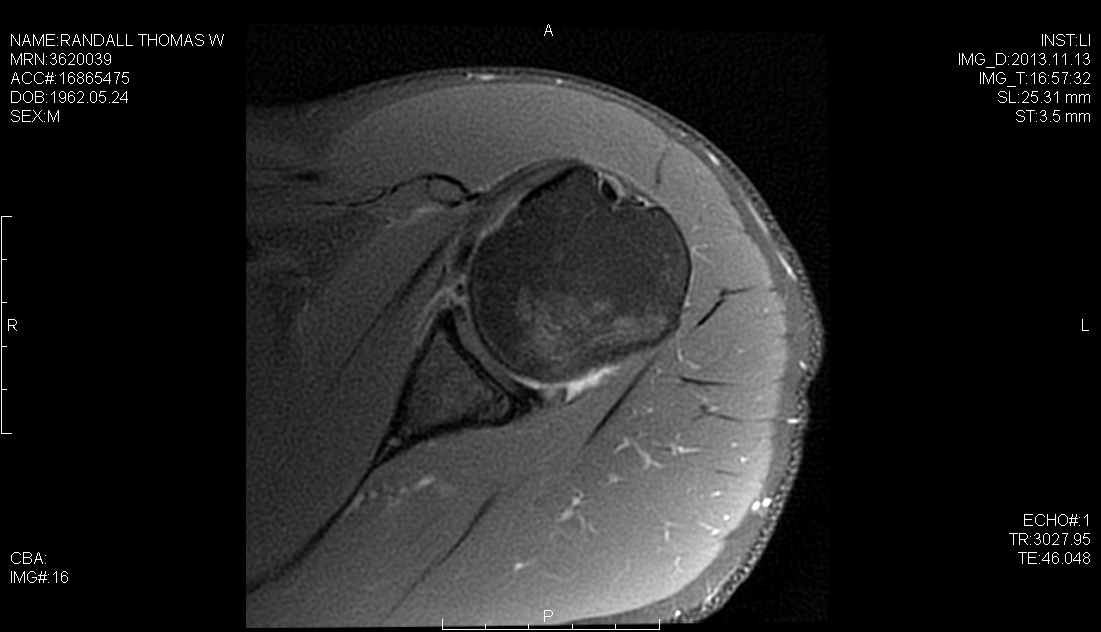 Axial T1 Weighted
Axial T1 Weighted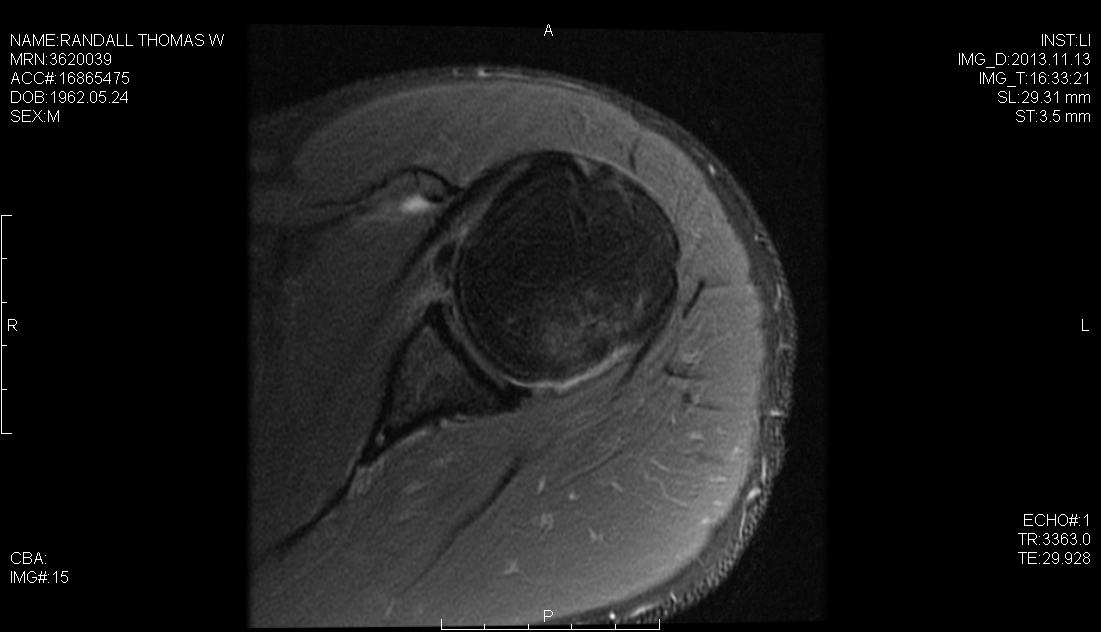 Axial Proton-density fat saturation
Axial Proton-density fat saturation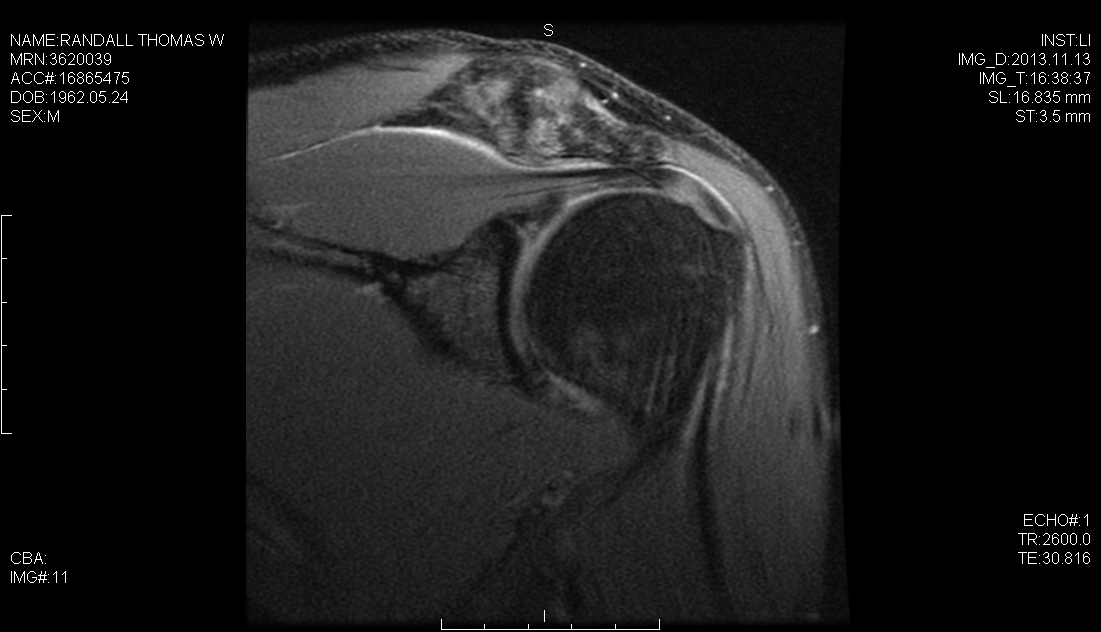 Coronal Proton-density fat saturation
Coronal Proton-density fat saturationNatural history
This patient developed anterior instability after traumatic dislocation in an anterior-inferior direction. Instability as the result of trauma almost always results from a labral tear which requires surgical intervention. Associated injuries may include superior labrum anterior-posterior (SLAP) lesions, rotator cuff tears, Hill-Sachs lesions, an Anterior Labral Periosteal Sleeve Avulsion (ALPSA) lesion, Humeral Avulsion of the Glenohumeral Ligament (HAGL) lesion, and a Glenoid labral articular defect (GLAD).Options for treatment
The options for treatment are conservative treatments including physical therapy and NSAIDs. Open surgical repair is still considered the gold standard, however arthroscopic management has certain advantages over open repair in the hands of a skilled surgeon. Open repair is indicated for a bony Bankart lesion greater than 20% of the glenoid. HAGL lesions are technically challenging to address arthroscopically and can be considered an indication for open repair.Rationale for this procedure
An arthroscopic repair compared to an open surgical procedure results in a shorter recovery and rehabilitation time, a decreased risk of joint infection, less risk of bleeding and the ability to visualize the entire shoulder joint with the arthroscope. An arthroscopic procedure also results in less pain during the recovery process.Special considerations
Patients with large bone defects or developmental abnormalities of the shoulder with dysplasia may require a more extensive, open approach. Normal neurologic function of the upper extremity is a necessity for a successful outcome. Failure of the patient to comply with the recommended postoperative restrictions and therapy protocols could result in a failure of the repair necessitating reoperation. Other complications from failure to follow the postoperative protocol could lead to infection, shoulder stiffness, or an otherwise sub-optimal result.Discussion
Technical advances in arthroscopic instability repair have led to outcomes approaching those of open surgical repair. Our approach to the arthroscopic Bankart uses the posterolateral portal described above in the technique section as the standard arthroscopic portals provide insufficient visualization and instrumentation access to the inferior glenoid.2 The advantages of the posterolateral portal are enhanced ability to place anchors in the inferior glenoid at an improved trajectory, improved anteroinferior knot tying, facilitation of anteroinferior labral repair, and anatomic reduction of the inferior glenohumeral ligament.Benefits and Limitations of Posterolateral Portal
In 2002 Davidson and Rivenburgh3 first described the 7 o'clock posterolateral portal in cadaveric shoulders as a way to obtain improved working access to the inferior glenoid. This portal entered the glenohumeral joint through the teres minor tendon at a safe distance from the suprascapular nerve and artery (28 ± 2 mm) and from the axillary nerve and posterior circumflex humeral artery (39 ± 4 mm).3 Difelice et al4 found in a cadaveric study that a similarly placed posterolateral portal had a distance of 34 ± 5 mm from the axillary nerve and 29 ± 3 mm from the suprascapular nerve. These studies also found that arm position did not change the distance from the portal to the neurovascular structures.3,4 The reported uses of the posterolateral portal include arthroscopic management of humeral avulsion of the glenohumeral ligament,5 posterior instability,6 and Bankart lesions.Outcomes
Outcomes of arthroscopic repair of Bankart lesions are favorable. Netto et al8 reported the results of a randomized controlled trial of 50 adult patients under 40 years of age with traumatic anterior shoulder instability and the presence of an isolated Bankart lesion confirmed by diagnostic arthroscopy, randomly assigned to receive open or arthroscopic treatment of an isolated Bankart lesion. The primary outcomes included the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaires. 42 patients were evaluated after a mean follow-up period of 37.5 months. On the DASH scale, there was a statistically significant difference favorable to the patients treated with the arthroscopic technique, but without clinical relevance. There was no difference in the assessments by University of California, Los Angeles and Rowe scales. There was no statistically significant difference regarding complications and failures, as well as range of motion, for the two techniques.Waterman et al retrospectively analyzed the outcomes of 3,854 active duty military patients who underwent Bankart repair between 2003 and 2010 with most procedures having been performed arthroscopically (n=3,230, 84%).9 Patients were predominantly men (n=3,531, 92%), and the mean age was 28.0 years (SD, 7.5 years). Younger age, open repair, and inpatient status were found to be risk factors for surgical failure. Patients who underwent arthroscopic Bankart repair had a significantly lower surgical failure rate (4.5%) than patients who underwent open anterior stabilization (7.7%).Possible Complications
- Recurrent instability
- Stiffness
- Infection
- Neurovascular injury
Equipment
- Spectrum MVP suture passer ConMed Linvatec, Largo, FL
- 3.0mm Suture Tak Anchors, Arthrex, Naples, FL
- 2.9mm PEEK Knotless Labral Tape Anchor, Arthrex, Naples, FL
- 0 PDS Sutures, Ethicon, Somerville, NJ
Disclosures
The author has no financial relationship with any of the companies mentioned in this article.Statement of Consent
The patient undergoing the filmed procedure gave consent to being filmed for this video article and is aware that it may be published online.References
- Seroyer ST, Nho SJ, Provencher MT, Romeo AA. Four-quadrant approach to capsulolabral repair: an arthroscopic road map to the glenoid. Arthroscopy. 2010;26(4):555-562. doi:10.1016/j.arthro.2009.09.019.
- Nord KD, Brady PC, Yazdani RS, Burkhart SS. The anatomy and function of the low posterolateral portal in addressing posterior labral pathology. Arthroscopy. 2007;23(9):999-1005. doi:10.1016/j.arthro.2007.04.011.
- Davidson PA, Rivenburgh DW. The 7-o'clock posteroinferior portal for shoulder arthroscopy. Am J Sports Med. 2002;30(5):693-696. doi:h10.1177/03635465020300051101.
- Difelice GS, Williams RJ III, Cohen MS, Warren RF. The accessory posterior portal for shoulder arthroscopy: description of technique and cadaveric study. Arthroscopy. 2001;17(8):888-891. doi:10.1016/S0749-8063(01)90015-5.
- Parameswaran AD, Provencher MT, Bach BR Jr, Verma N, Romeo AA. Humeral avulsion of the glenohumeral ligament: injury pattern and arthroscopic repair techniques. Orthopedics. 2008;31(8):773-779. doi:10.3928/01477447-20080801-21.
- Bradley JP, Tejwani SG. Arthroscopic management of posterior instability. Orthop Clin North Am. 2010;41(3):339-356. doi:10.1016/j.ocl.2010.02.002.
- Baker CL III, Romeo AA. Combined arthroscopic repair of a type IV SLAP tear and Bankart lesion. Arthroscopy. 2009;25(9):1045-1050. doi:10.1016/j.arthro.2009.04.075.
- Archetti Netto NA, Tamaoki MJS, Lenza M, et al. Treatment of Bankart lesions in traumatic anterior instability of the shoulder: a randomized controlled trial comparing arthroscopy and open techniques. Arthroscopy. 2012;28(7):900-908. doi:10.1016/j.arthro.2011.11.032.
- Waterman BR, Burns TC, McCriskin B, Kilcoyne K, Cameron KL, Owens BD. Outcomes after Bankart repair in a military population: predictors for surgical revision and long-term disability. Arthroscopy. 2014;30(2):172-177. doi:10.1016/j.arthro.2013.11.004.
Cite this article
Provencher M. Arthroscopic Bankart repair for anterior shoulder instability using a posterolateral portal. J Med Insight. 2014;2014(5). doi:10.24296/jomi/5.
