
Arthroscopic ACL Reconstruction with Bone Patellar Bone Graft using Anteromedial Technique
Main Text
Table of Contents
Abstract
There are approximately 200,000 anterior cruciate ligament (ACL) injuries per year in the United States and more than half will be treated with ACL reconstruction. The diagnosis is made by physical exam supplemented by radiographs and MRI scan. Successful ACL reconstruction returns most athletes to pre-injury activity; however, outcome depends on appropriate preoperative evaluation, surgical timing, surgical technique, and an effective postoperative physical therapy program. Specifically, graft choice, graft positioning, and fixation technique have been shown to play important roles in patient outcome. Surgeons must also be aware of concomitant meniscal tears and cartilage injury that may need to be addressed at the time of ACL reconstruction. In the present case, we perform an anatomic ACL reconstruction with bone-patellar tendon-bone (BTB) autograft using an anteromedial drilling technique and flexible reamers for a young college athlete. The anteromedial approach offers the advantage of reliably reproducing the native anatomy of the ACL on the femur footprint by drilling the femoral tunnel independently of the tibial tunnel. Furthermore, using a flexible reamer instead of a straight rigid reamer allows for a longer femoral tunnel and lower risk of posterior wall blowout or fracture.
Case Overview
Focused History
This is a 19-year-old collegiate intramural athlete that sustained a non-contact injury of his right knee while playing ultimate Frisbee. He described twisting on his right knee when he heard a “pop”. He had a large joint effusion when he was initially evaluated at a local emergency department. He presented to our orthopedic office approximately one month after his injury. At that time, he had minimal pain but felt the knee “buckle” on him several times per week. He was unable to return to his pre-injury level of participation as an active collegiate student involved in intramural athletics.
Physical Exam
On exam, this patient had a moderate knee effusion and could flex his knee from 0 to 130 degrees. He had mild tenderness over the lateral joint line with slight opening of 5 degrees with valgus stress at 0 degrees but not at 30 degrees. His knee was stable to varus stress. He had a grade 2B Lachman test with a positive pivot shift. The dial test in the prone position at 30 and 90 degrees of knee flexion was symmetrical. He had normal sensation and blood flow to the lower extremity.
Imaging
Initial imaging consists of a knee trauma radiograph series including anteroposterior, lateral and patellar views.1 The images should be closely reviewed for bony avulsion fractures and any associated bony injuries. The Segond sign (small avulsion off the lateral tibial plateau) represents a lateral capsular avulsion which should raise suspicion for an ACL rupture.2 In select patients at risk for knee osteoarthritis, posterior to anterior, 45 degree flexion weight-bearing films may be obtained.3 Knee MRI is the most sensitive and specific in diagnosing ACL injuries. Bone contusions of the lateral femoral condyle and posterior tibial plateau are the most common associated finding.4 Injuries to the menisci, collateral ligaments and posterior cruciate ligament are also reliably detected on MRI. Knowledge of concomitant knee injuries is essential for preoperative planning.
Natural History
This patient has recurrent episodes of symptomatic knee instability following his initial injury. The medial collateral ligament and menisci are often injured at the time of initial injury with lateral meniscus injuries more common acutely. Untreated ACL injuries may lead to further chondral and meniscal injuries. It is unclear if ACL reconstruction will reduce the incidence of arthritis.5, 6
Options for Treatment
Treatment options include physical therapy starting with an emphasis on reestablishing full range of motion (flexion and extension) and controlling the effusion followed by quadriceps and hamstring strengthening. Then, a sport-specific rehabilitation protocol may be initiated. For high demand athletes and active patients with symptoms of instability, surgical ACL reconstruction is recommended. Both open and arthroscopic techniques exist with multiple graft choices including autograft (BTB, quadrupled hamstring, quadriceps tendon) and allograft (semitendinosis, Achilles tendon, BTB, tibialis anterior, tibialis posterior).
Rationale for This Procedure
Compared to open surgery, arthroscopic ACL reconstruction is associated with a shorter recovery and rehabilitation time with a decreased risk of infection. Partial meniscectomy, meniscal repair, and procedures for cartilage damage can be performed simultaneously. Autograft tissue is associated with a decreased re-rupture rate in young athletes when compared to allograft tissue.7 ACL reconstruction with BTB autografts have similar clinical outcomes when compared to the use of hamstring autografts. However, recent clinic studies have shown decreased failure rate with BTB autograft and a more stable knee on KT 1000 testing.8 Furthermore, the anteromedial approach for ACL reconstruction offers the advantage of reliably reproducing the native anatomy of the ACL femoral footprint by drilling the femoral tunnel independently of the tibial tunnel. Historically, this has been challenging to accomplish with a transtibial technique. We propose that using a flexible reamer instead of a straight rigid reamer allows for a longer femoral tunnel and lower risk of posterior wall blowout or fracture.
Equipment
- AcuFex Anatomic ACL Instrumentation by Smith and Nephew, Andover, MA
- Stryker Flexible ACL Versitomic drills
- Stryker Metal Interference screws.
Special Considerations and Contraindications to ACL Surgery
Absolute contraindications to arthroscopic ACL reconstruction include any patient with an active knee infection or who is unfit for anesthesia. Relative contraindications include patients who are unlikely to follow post-operative rehabilitation protocols. Failure to comply with rehabilitation may result in arthrofibrosis and a poor outcome. Relative contraindications to patellar tendon harvest include patients who have preexisting anterior knee pain, jobs that require kneeling (Clergy, carpenters), jumping sport athletes, older patients, and those with narrow patellar tendons or patellar chondrosis.
Patient Follow-Up
At 4 months post-operatively, our patient has pain free range of motion from 0 to 130 degrees of knee flexion with a grade 1A Lachman test, a negative pivot shift, and no varus or valgus instability.
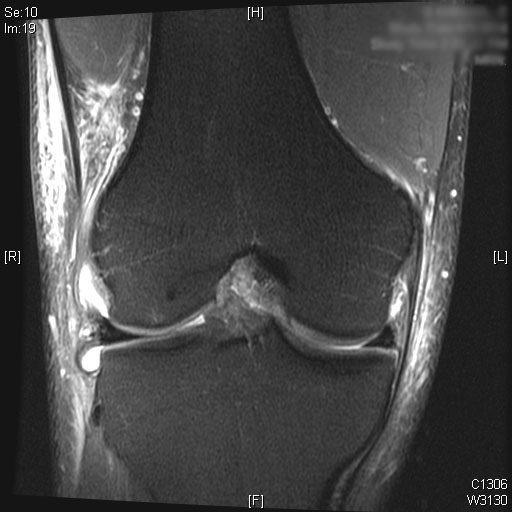
Pre-Op X-Rays and MRI
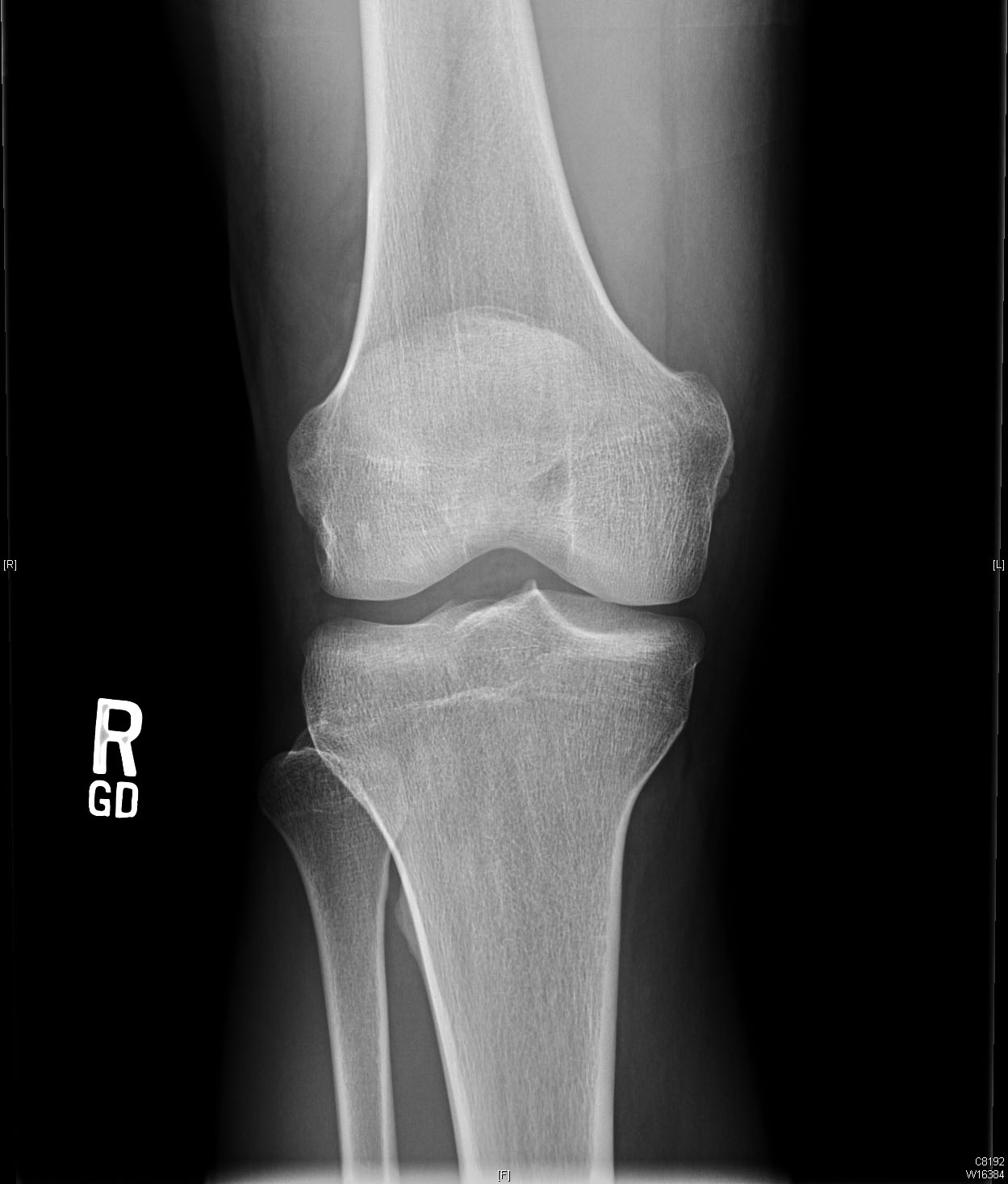
Pre-operative radiographs shows slight anterior translation of the tibia in relation to the femur on the lateral image.

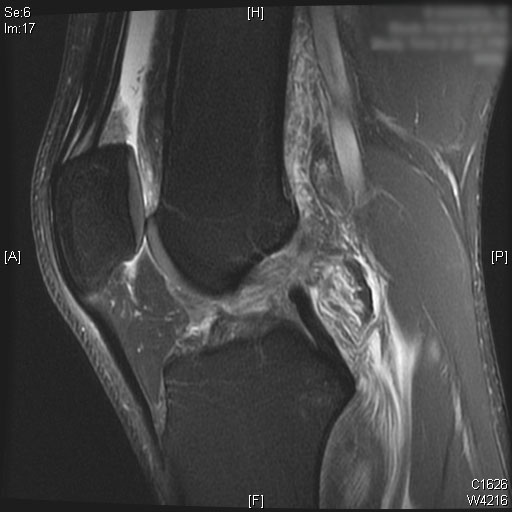
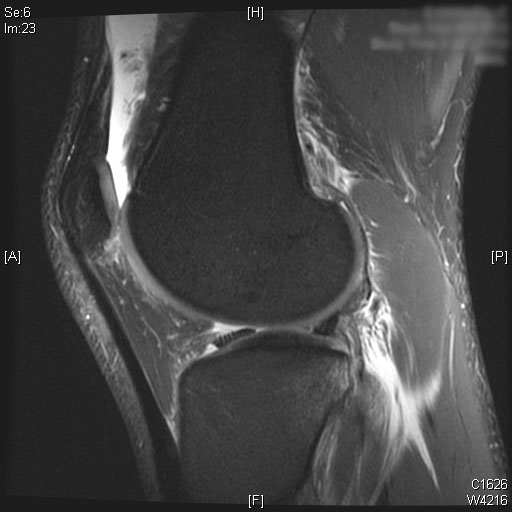
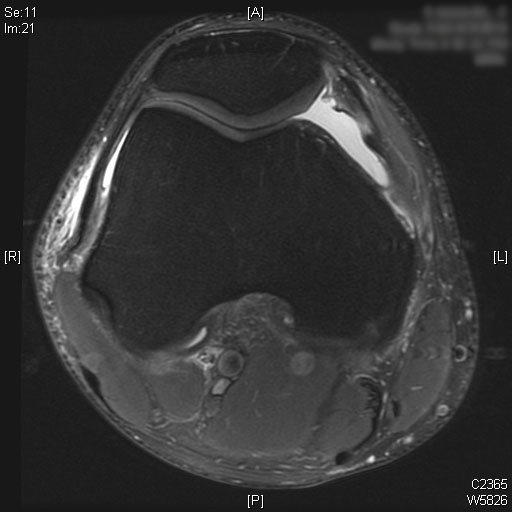
Complete ACL rupture is seen on the sagittal T2 MRI images. Also, bone marrow edema is seen on the posterior third of the lateral tibial plateau. Cartilage on the medial and lateral femoral condyle alone with the patella is preserved. Moderate joint effusion is visualized on the T2 MRI images.



Post-Op X-Rays


Discussion
ACL reconstruction for ACL ruptures is associated with a high rate of return to sports performance and improved knee functional scores.9 In patients who wish to return to sports, reconstructing the ACL has been shown to reduce the rate of further osteochondral and meniscal injury.5, 6
Femoral tunnel placement has been an issue of debate with many published studies. Recent literature suggests that a lower lateral tunnel in the 10:30 or 1:30 position will more accurately recreate the position and function of the natural ACL, especially the rotational stability. This anatomic femoral tunnel position can be achieved with the use of an anteromedial portal and straight reamers, flexible reamers, and even the transtibial technique with hyperflexion of the knee.10 Historically, traditional transtibial ACL reconstruction techniques resulting in a vertical ACL graft have been associated with improved knee stability in the anterior to posterior plane, but with persistence of rotational instability and a positive pivot shift.8, 11 Biomechanically, double bundle ACL reconstruction where both the anteromedial and posterolateral bundles are reconstructed will most closely reproduce natural ACL function. However, Adachi et al. failed to show any clinical difference between a single bundle and double bundle technique in a prospective randomized controlled trial of 108 patients.12 Until a clear clinical benefit for double bundle anatomic ACL reconstruction is demonstrated, we prefer a single bundle anatomic technique that is achieved by using an anteromedial portal and flexible reamers for femoral tunnel drilling.
Altentorn-Geli et al. compared the clinical outcome data of patients after ACL reconstruction using a transtibial (TT) technique compared to an anteromedial (AM) technique. The authors reported significantly faster recovery time from surgery, walking without crutches, and return to normal life with the AM technique. In addition, patients in the AM ACL reconstruction group had significantly better knee stability (KT-1000, pivot-shift test, Lachman test, and IKDC scores) compared to the TT group. Koutras et al. also showed better Lysholm knee scores and performance in patients after AM ACL reconstruction compared to a TT technique with short-term follow-up.13 Furthermore, Mardani-Kivi et al. also reported significantly faster return to activity, better range of motion, and greater patient satisfaction in the AM ACL reconstruction group. However, he did not show a difference in Lachman testing or knee stability.14
In addition, the use of an autograft construct has been shown to have a decreased rate of re-rupture in young active athletes compared to allograft.7 We reserve allografts for older (> 40 years of age), low demand patients or for revision cases where autograft choices may be limited. Patellar tendon grafts have less laxity (KT-1000) compared to hamstring grafts and some studies have also demonstrated lower failure rates.15 However, BTB grafts are associated with slightly higher rates of anterior knee pain.
Tips for History:
- Obtain a medical history including the mechanism of injury, previous injuries, type of sport and activity level
- When and how did the injury occur? What was the mechanism?
- What symptoms do you currently experience? Is there pain or instability? What limitations in activity have occurred as a result of injury?
- What prior treatments has the patient tried (physical therapy, activity modification, medications)?
Tips for Physical Exam:
- Visually inspect the knee for an effusion, ecchymosis, and the condition of the skin.
- Carefully palpate the knee joint. Joint line tenderness may indicate a meniscus injury. Any defect in the extensor mechanisms or extensor lag may be indicative of an extensor mechanism injury.
- Evaluate active and passive knee range of motion. Any loss of passive extension may be due to a displaced bucket handle meniscus tear or arthrofibrosis. Loss of flexion may result from significant knee effusion.
- The knee should be stressed with a varus and valgus force at 0 and 30 degrees of flexion to detect collateral ligament injuries. Any instability at 0 degrees correlates with a collateral ligament injury with rupture of one or both cruciate ligaments.
- Injuries to the posterior cruciate ligament and posterolateral corner should be tested for with the posterior drawer test and the external rotation dial test in the prone position, respectively.
- Patellar instability can also be assessed with apprehension testing by applying a laterally direct force on the patella with the leg in 20 to 30 degrees of flexion. In this position, the patella is engaged in the trochlea groove.
- Tests for anterior cruciate ligament (ACL) rupture
- The Lachman test is performed with the knee flexed 20 to 30 degrees with one hand stabilizing the femur. The other hand is then used to apply an anterior force on the tibia from a neutral starting position. Laxity is compared to the contralateral side. The test can be graded according to the degree of anterior displacement.1 Grade 1 is up to 5mm difference, Grade 2 is 5 to 10mm, and Grade 3 is > 10mm of anterior translation. The letter ‘A’ is applied after the grade if a firm endpoint is present with anterior translation while the letter ‘B’ is applied if there is no firm endpoint.
- The Pivot shift test can be used to assess the degree of rotational knee dysfunction. It is difficult to perform clinically, but is very sensitive during examination under anesthesia.2, 3 With the patient supine, the affected leg is slightly abducted to relax the iliotibial band. Then, an internal rotation and valgus force is applied while the examiner passively flexes the knee. In an ACL deficient patient, a positive pivot shift is typically detected from 20 to 40 degrees of flexion, which is when the anterior subluxated tibia is reduced by the iliotibial band.
- In the ACL deficient knee, the knee will subluxate anteriorly between 20 and 40 degrees of flexion. A positive pivot shift test is typically detected between 20 and 40 degrees of flexion, which is when the anterior subluxated tibia is reduced by the iliotibial band.
Overall Outcomes After ACL Reconstruction
Outcomes for ACL reconstruction are favorable with success rates of up to 95%. In a retrospective review of 97 patients by Bach et al., 70% of patients had less than 3-mm on KT-1000 arthrometer testing. The same group also reported significant improvements in Teneger activity level, a mean Lysholm score of 87, and good to excellent modified Hospital for Special Surgery scores for 82% of patients.13 A review of recent literature by Chalmers of studies with more than 10 years of follow-up compared cohorts of 685 patients treated nonoperatively and 1585 patients treated with ACL reconstruction. The operative group had significantly improved activity levels according to the Tegner score, fewer subsequent meniscal injuries, and significantly fewer additional knee operations. However, they did not identify any difference in the Lysholm score, the IKDC score or the development of radiographically evident osteoarthritis.14
In active patents with an ACL tear, early ACL reconstruction may be more cost effective than delayed treatment after physical therapy. Mather et al. used the Multicenter Orthopaedic Outcomes Network (MOON) database to show that early ACL reconstruction was more effective in improved quality-adjusted life-years gained at a lower cost compared to optional delayed reconstruction after a period of rehabilitation.15
Future Research
With increasing numbers of young at risk athletes, future research is turning to injury prevention. Multiple recent studies have noted the ability of injury prevention and neuromuscular training to reduce the incidence of ACL ruptures. Cost-effectiveness studies Sadoghi et al. and Swart et al. demonstrated that universal neuromuscular training is the most cost effective method of ACL injury prevention.16, 17
Disclosures
The author has no financial relationship with any of the companies mentioned in this article.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
References
- Torg JS, Conrad W, Kalen V. Clinical diagnosis of anterior cruciate ligament instability in the athlete. Am J Sports Med. 1976;4(2):84-93. doi:10.1177%2F036354657600400206.
- Fetto JF, Marshall JL. Injury to the anterior cruciate ligament producing the pivot-shift sign. J Bone Joint Surg Am. 1979;61(5):710-714. doi:10.2106/00004623-197961050-00010.
- Bach BR Jr, Warren RF, Wickiewicz TL. The pivot shift phenomenon: results and description of a modified clinical test for anterior cruciate ligament insufficiency. Am J Sports Med. 1988;16(6):571-576. doi:10.1177%2F036354658801600603.
- Yoon KH, Yoo JH, Kim KI. Bone contusion and associated meniscal and medial collateral ligament injury in patients with anterior cruciate ligament rupture. J Bone Joint Surg Am. 2011;93(16):1510-1518. doi:10.2106/JBJS.J.01320.
- Fithian DC, Paxton EW, Stone ML, et al. Prospective trial of a treatment algorithm for the management of the anterior cruciate ligament-injured knee. Am J Sports Med. 2005;33(3):335-346. doi:10.1177/0363546504269590.
- Daniel DM, Stone ML, Dobson BE, Fithian DC, Rossman DJ, Kaufman KR. Fate of the ACL-injured patient: a prospective outcome study. Am J Sports Med. 1994;22(5):632-644. doi:10.1177%2F036354659402200511.
- Pallis M, Svoboda SJ, Cameron KL, Owens BD. Survival comparison of allograft and autograft anterior cruciate ligament reconstruction at the United States Military Academy. Am J Sports Med. 2012;40(6):1242-1246. doi:10.1177/0363546512443945.
- Spindler KP, Huston LJ, Wright RW, et al. The prognosis and predictors of sports function and activity at minimum 6 years after anterior cruciate ligament reconstruction: a population cohort study. Am J Sports Med. 2011;39(2):348-359. doi:10.1177/0363546510383481.
- Loh JC, Fukuda Y, Tsuda E, Steadman RJ, Fu FH, Woo SL. Knee stability and graft function following anterior cruciate ligament reconstruction: comparison between 11 o'clock and 10 o'clock femoral tunnel placement. Arthroscopy. 2003;19(3):297-304. doi:10.1053/jars.2003.50084.
- Woo SL, Kanamori A, Zeminski J, Yagi M, Papageorgiou C, Fu FH. The effectiveness of reconstruction of the anterior cruciate ligament with hamstrings and patellar tendon: a cadaveric study comparing anterior tibial and rotational loads. J Bone Joint Surg Am. 2002;84(6):907-914. doi:10.2106/00004623-200206000-00003.
- Musahl V, Plakseychuk A, VanScyoc A, et al. Varying femoral tunnels between the anatomical footprint and isometric positions: effect on kinematics of the anterior cruciate ligament-reconstructed knee. Am J Sports Med. 2005;33(5):712-718. doi:10.1177/0363546504271747.
- Adachi N, Ochi M, Uchio Y, Iwasa J, Kuriwaka M, Ito Y. Reconstruction of the anterior cruciate ligament. Single- versus double-bundle multistranded hamstring tendons. J Bone Joint Surg Br. 2004;86(4):515-520. doi:10.1302/0301-620X.86B4.14856.
- Bach BR Jr, Tradonsky S, Bojchuk J, Levy ME, Bush-Joseph CA, Khan NH. Arthroscopically assisted anterior cruciate ligament reconstruction using patellar tendon autograft. Am J Sports Med. 1998;26(1):20-29. doi:10.1177/03635465980260012101.
- Chalmers PN, Mall NA, Moric M, et al. Does ACL reconstruction alter natural history?: A systematic literature review of long-term outcomes. JBJS. 2014;96(4):292-300. doi:10.2106/JBJS.L.01713
- Mather III RC, Hettrich CM, Dunn WR, et al. Cost-effectiveness analysis of early reconstruction versus rehabilitation and delayed reconstruction for anterior cruciate ligament tears. Am J Sports Med. 2014;42(7):1583-91. doi.org/10.1177/0363546514530866
- Sadoghi P, von Keudell A, Vavken P. Effectiveness of anterior cruciate ligament injury prevention training programs. J Bone Joint Surg Am. 2012;94(9):769-776. doi:10.2106/JBJS.K.00467
- Swart E, Redler L, Fabricant PD, Mandelbaum BR, Ahmad CS, Wang YC. Prevention and screening programs for anterior cruciate ligament injuries in young athletes: a cost-effectiveness analysis. J Bone Joint Surg Am. 2014;96(9):705-711. doi:10.2106/JBJS.M.00560.
Cite this article
Li X, Orvets ND. Arthroscopic ACL reconstruction with bone patellar bone graft using anteromedial technique. J Med Insight. 2016;2016(45). doi:10.24296/jomi/45.

