
Left Laparoscopic Transperitoneal Adrenalectomy for Aldosteronoma
Main Text
Table of Contents
Abstract
Primary hyperaldosteronism refers to the autonomous secretion of the hormone aldosterone from the adrenal gland, resulting in low renin levels. This usually occurs in individuals between the ages of 30 to 50 years old. The majority of these cases are caused either by a solitary, functioning adrenal adenoma or aldosteronoma (70%) or by idiopathic bilateral hyperplasia (30%). Other uncommon causes include adrenal carcinoma and familial hyperaldosteronism. Patients typically present with hypokalemia and long-standing hypertension that is difficult to control despite multi-drug therapy; nevertheless, further tests are required for diagnosis. An elevated plasma aldosterone level with a suppressed plasma renin level is strongly suggestive of the diagnosis. Once confirmed, further evaluation should be directed toward determining if the cause is a unilateral aldosteronoma or bilateral adrenal hyperplasia. This is done through imaging studies and adrenal vein sampling. Unilateral aldosteronoma is best managed by adrenalectomy, with the laparoscopic approach being the preferred method. Bilateral adrenal hyperplasia is often best treated medically because only 20–30% benefit from surgery. Here, we present the case of a 48-year-old woman who had long-standing hypertension and hypokalemia and was found to have hyperaldosteronism and low renin levels. A CT scan showed a small mass in the left adrenal gland, and adrenal vein sampling showed higher levels of aldosterone on the left side than on the right, confirming a unilateral aldosteronoma. Laparoscopic access was gained, the adrenal gland was exposed and dissected by controlling the periadrenal tissues with the harmonic scalpel, the adrenal vein was then ligated, and the adrenal gland was removed.
Case Overview
Background
Primary aldosteronism, or Conn’s syndrome, was first described in 1956.1 It is a common cause of secondary hypertension, accounting for between 1–10% of all patients with hypertension. The pathophysiology involves hypersecretion of aldosterone, either by primary aldosterone-producing tumors or by hyperplasia of the zona glomerulosa of the adrenal gland.2
Primary hyperaldosteronism is diagnosed by measuring aldosterone, renin, and potassium levels. Typically, patients have high aldosterone levels, low renin levels, and low potassium levels. Following laboratory investigations, it is imperative to locate the source of the excess aldosterone. This is often achieved with imaging studies. Adrenal vein sampling is also generally performed to determine the side that is producing excess aldosterone, especially in cases where imaging may be inconclusive. Primary hyperaldosteronism that is caused by an adrenal gland tumor is treated with adrenalectomy. Virtually 100% of patients experience normalization of their hypokalemia following successful surgery. Fewer, though still the majority, experience at least some degree of lowering of their blood pressure.
Focused History of the Patient
The patient is a 48-year-old woman who has long-standing hypertension, for which she had been treated with several medications. She was also noted to have hypokalemia, and eventually was sent to an endocrinologist who did appropriate blood testing to biochemically confirm that she had hyperaldosteronism with suppressed renin levels. She was therefore diagnosed with aldosteronism.
The patient had a CT scan showing a small left-sided adrenocortical adenoma. She then underwent adrenal vein sampling. This confirmed excess aldosterone secretion on the left side with a very high aldosterone/cortisol ratio compared to the right side (aldo/cortisol ratio of >3, left:right).
Physical Exam
There are no particular physical signs or symptoms of primary aldosteronism; however, chronic hypertension often results in left ventricular hypertrophy. This may be heard on auscultation as an S4 sound. The examiner may also hear carotid bruits. On neurological exam, there may be muscular weakness (secondary to hypokalemia) and mental status changes associated with hypertensive encephalopathy.
Imaging
A CT scan revealed a small nodule in the left adrenal gland (Figure 1). The right-sided adrenal appeared normal. This finding, combined with adrenal vein sampling, strongly suggested that the patient should have her left adrenal gland removed.
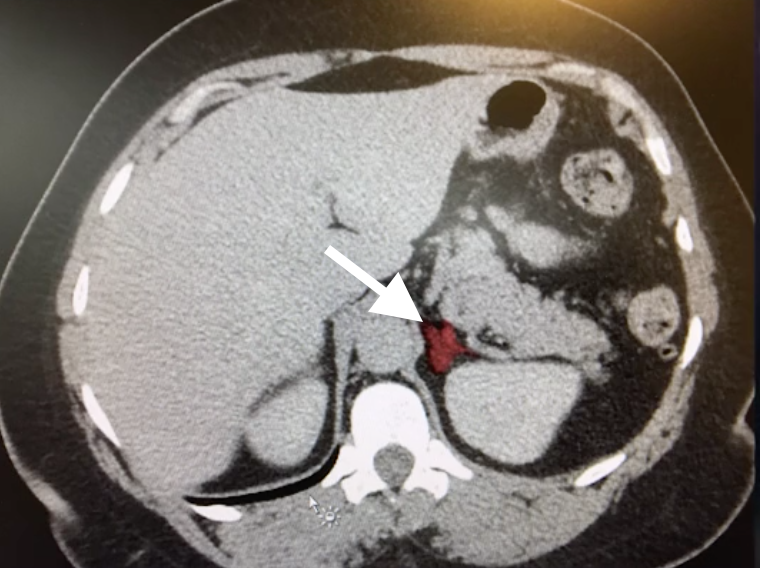
Figure 1. Abdominal CT Non-contrast CT image revealing a lesion (white arrow) in the area of the left adrenal gland.
Natural History
Primary hyperaldosteronism is characterized by sequelae of hypokalemia and chronic hypertension. Muscle weakness, periodic paralysis and elevated serum creatine kinase levels secondary to hypokalemia have been reported prior to the detection of elevated blood pressure.3 Patients with long-standing hypertension are exposed to higher risks of major adverse cardiac events, including stroke, myocardial infarction, and atrial fibrillation.2
Options for Treatment
For patients with medication-resistant hypertension, a work-up for Conn’s syndrome is indicated. If a unilateral tumor is identified as the source of the excess aldosterone, surgery to remove the tumor is indicated. The options are most often laparoscopic or retroperitoneal procedures. These minimally-invasive procedures rarely need to be converted to open procedures.
Rationale for Treatment
There are two reasons to remove these tumors: to correct the hypokalemia and to relieve the hypertension. The procedure reverses hypokalemia in virtually 100% of cases; however, patients are able to discontinue anti-hypertensive medications in only 35% of cases. This is likely because hypertension is often multifactorial (e.g., there may be an element of essential hypertension as well) or there may be occult disease on the contralateral side.4
Special Considerations
Laparoscopic adrenalectomy is most effective when the disease is unilateral. Surgery is generally contraindicated in patients with bilateral disease; these patients are best treated medically with anti-hypertensives, especially mineralocorticoid-blocking agents such as spironolactone.
Discussion
Our patient underwent a successful resection of her left adrenal gland. The unusual features of the case included our finding of substantial amounts of adhesions in her abdomen without obvious cause. The tumor itself appeared hemorrhagic on gross examination. This is unusual in an aldosteronoma.
Most patients are able to go home either the same day or with a short < 24 hour hospital admission, provided they have no significant comorbidities. We decreased this patient’s blood pressure medications and had her monitor her blood pressure at home twice per day. We follow-up patients closely with telephone calls after the surgery and ensure that their blood pressure readings are monitored along with the serum potassium levels. We are confident that her potassium levels will normalize. It remains to be seen whether she will become normotensive, as she has other risk factors for hypertension, including obesity.
Equipment
- Endo Catch Bag
Disclosures
Nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
References
- Conn JW, Louis LH. Primary aldosteronism, a new clinical entity. Annals of internal medicine. 1956 Jan 1;44(1):1-5. doi:10.7326/0003-4819-44-1-1.
- Cobb A, Aeddula NR. Primary hyperaldosteronism. [Updated 2019 Apr 21]. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2019. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539779/?report=classic.
- Olt S, Yaylaci S, Tatli L, Gunduz Y, Garip T, Tamer A. Hypokalemia-induced myopathy and massive creatine kinase elevation as first manifestation of Conn's syndrome. Niger Med J. 2013;54(4):283. doi:10.4103/0300-1652.119658.
- Parthasarathy HK, Ménard J, White WB, et al. A double-blind, randomized study comparing the antihypertensive effect of eplerenone and spironolactone in patients with hypertension and evidence of primary aldosteronism. J Hypertens. 2011 May;29(5):980-90. doi:10.1097/HJH.0b013e3283455ca5.
Cite this article
Hodin R. Left laparoscopic transperitoneal adrenalectomy for aldosteronoma. J Med Insight. 2023;2023(182). doi:10.24296/jomi/182.
