
Combined Thymectomy and Right Lower Lobe Pulmonary Wedge Resection by Thoracoscopy
Main Text
Table of Contents
Abstract
With the increasing use of computed tomography (CT) for screening and diagnostic workup, increasing numbers of patients are found to have pulmonary nodules. The patient in this case presented with vision changes, neck weakness, and dysphagia. Workup revealed non-thymomatous myasthenia gravis as well as an incidental right lower lobe lung nodule that was suspicious for malignancy based on imaging characteristics, interval growth, and history of breast cancer. She required a lung resection for diagnostic and therapeutic purposes. Additionally, a thymectomy was indicated to help control her myasthenia gravis symptoms. Consequently, a combined approach was conducted.
Case Overview
Background
Myasthenia gravis (MG) is an autoimmune disorder in which autoantibodies directed at components in the postsynaptic membrane of the neuromuscular junction (acetylcholine receptors or receptor-associated proteins) result in fatigable weakness of ocular, bulbar, limb, or respiratory muscles. Most patients have detectable antibodies against the acetylcholine receptor or muscle-specific tyrosine kinase receptor.
Patients with MG present with fluctuating skeletal muscle weakness that is worse later in the day or after exercise. Ptosis and/or diplopia is the initial presentation in 50% of patients. A smaller proportion of patients present with bulbar symptoms such as dysarthria, dysphagia, and fatigable chewing and less frequently with proximal limb weakness. When respiratory muscle weakness leads to respiratory failure, this is termed “myasthenic crisis” and is a life-threatening situation. Myasthenic crisis can be precipitated by many factors including medications, surgery, or inflammation/infection.
Focused History of Patient
This is a 69-year-old female with a history of myasthenia gravis, hypertension, diabetes, left breast cancer treated with lumpectomy, adjuvant radiation, and hormonal therapy who presented with a right lower lobe spiculated lung nodule. The patient started having myasthenia symptoms about 1 year prior to presentation. She had diplopia, drooping head, unsteady gait, and dysphagia.
Physical Exam
On examination, patients demonstrate weak eye movements with intact pupil function. They may appear expressionless due to facial muscle involvement and have a “dropped head” from weak posterior neck muscles. This patient in this scenario had clear lung sounds bilaterally. She had fatigable bilateral ptosis, right greater than left. She had fatigable left hyperopia in extraocular movements. She had decreased neck flexion strength. The rest of the neurological examination was unremarkable.
Imaging Studies
The diagnosis of MG can be confirmed by serologic tests for autoantibodies and electromyographic studies. The edrophonium chloride (Tensilon) test is sensitive but has a significant false positive rate. A chest CT or MRI should be obtained to demonstrate the absence of a thymoma. About 60–70% of MG patients have thymic hyperplasia, and 10–15% of patients have an underlying thymoma.
In this case, a chest CT revealed a spiculated 1.3-cm lesion at the fissural surface of the superior segment in the right lower lobe that was highly suspicious for a carcinoma of the lung (Figure 1). A PET/CT was subsequently obtained that showed FDG avidity suspicious for malignancy.
 Figure 1A. CT chest image in axial view.
Figure 1A. CT chest image in axial view.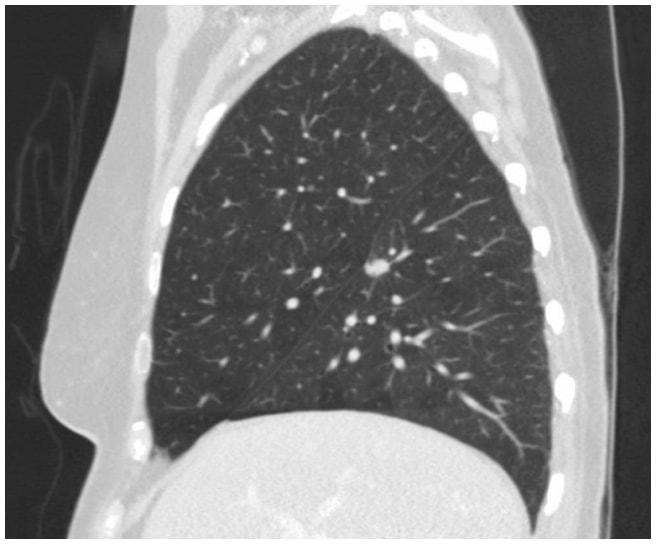 Figure 1B. CT chest image in sagittal view.
Figure 1B. CT chest image in sagittal view.Natural History
The natural history of MG is that of progressively shorter symptom-free intervals that peak within 2 to 3 years of disease onset. A period of time then elapses when patients typically have a persistent, stable disease that can worsen in the setting of infection, medications, or other clinical changes. A third phase may follow in which about 10–20% of patients may have spontaneous remission.
Options for Treatment
Medical management of MG involves symptom control (anticholinesterase agents) and immunomodulation (steroids, immunosuppression, plasma exchange, intravenous immunoglobulin). Patients with non-thymomatous MG may benefit from thymectomy to improve symptoms or increase the probability of disease remission. The Myasthenia Gravis Foundation of America (MGFA) classification of MG severity suggests that patients with only ocular MG (MGFA I) do not derive benefit from thymectomy whereas patients with generalized MG (MGFA >II) may see symptom improvement.1 An important caveat is that a high percentage (50–70%) of patients with ocular MG progress to generalized MG over the first 2 to 3 years of diagnosis; thus, early thymectomy may “rescue” a proportion of this population.
Rationale for Treatment
This patient had a right lower lobe lung nodule that was suspicious for malignancy and non-thymomatous myasthenia gravis. She required a lung resection for diagnostic and therapeutic purposes as well as a thymectomy to help control her myasthenia gravis symptoms. Consequently, a combined approach was conducted.
Transcervical thymectomy is the least invasive open approach; however, complete resection of perithymic tissue is limited. This is important because the thymus may extend beyond its anatomic boundaries (innominate vein superiorly and phrenic nerves laterally), and about 75% of patients have ectopic thymic tissue throughout the anterior mediastinum. Minimally-invasive techniques such as video-assisted thoracoscopic (VATS) or robotic thymectomy result in improved visualization and completeness of resection. They are performed either from the left or the right chest depending on surgeon preference and tumor laterality.
Special Considerations
The surgeon should work with the neurologist to optimize the patient preoperatively to prevent postoperative myasthenic crisis and avoid respiratory failure. Forced vital capacity and maximal breathing capacity (frequency multiplied by the volume of breaths in 1 minute) should be measured to assess respiratory weakness. MG symptoms must be well controlled with cholinesterase inhibitors, immunosuppression, plasmapheresis, or intravenous immunoglobulin treatment before operation.
Preoperative planning with the anesthetic team is critical; neuromuscular blockade is completely avoided as patients with MG are resistant to succinylcholine and highly, and unpredictably, sensitive to nondepolarizing agents. Sedatives and anesthetics should be short acting to minimize respiratory depression on emergence from anesthesia. A combination of inhalational and intravenous anesthesia is often used. Other medications known to interfere with neuromuscular transmission should be avoided.
MG symptoms improvement or remission after thymectomy may be seen several years after thymectomy.
Given the expectation of prolonged immunosuppressive therapy for MG, diagnosis of a solitary pulmonary nodule is desirable to exclude specific infection and aggressive neoplastic disease.
Pathology Report
A. LUNG WEDGE BIOPSY, RIGHT LOWER LOBE:
Carcinoid tumor, typical.
One lymph node in the wedge resection is involved by carcinoid tumor.
NOTE: The tumor cells are diffusely synaptophysin and chromogranin positive. A stain for ER is negative. Ki-67 stains 1% of tumor cells. One minute microscopic focus of cellular degeneration is present. Cytologic atypia is minimal. No mitoses are identified.
Tumor islands are present in some alveoli adjacent to the nodule of tumor. There is limited lymphangitic spread of tumor but not at resection margin. Margins of excision are free of tumor. A portion of the carcinoid tumor is densely sclerotic.
Some of the histologic features are unusual, but the findings do not constitute a diagnosis of atypical carcinoid tumor. Selected slides were reviewed in conference.
B. STATION 12 MAJOR FISSURE:
There is no evidence of malignancy in one lymph node (0/1).
C. STATION 12 LYMPH NODE BIOPSY:
Metastatic carcinoid tumor in one lymph node (1/1).
D. STATION 7 LYMPH NODE BIOPSY:
There is no evidence of malignancy in two lymph nodes (0/2).
E. THYMUS RESECTION:
Fatty replacement. No thymic tissue is identified.
Discussion
Thymectomy for MG was first described by Alfred Blalock in 1939 in the case of a young woman with a thymoma whose myasthenic symptoms went into remission after thymectomy.2 In 1941, he further demonstrated that symptom improvement could also be achieved in patients with non-thymomatous MG who underwent thymectomy.3 Thymectomy for MG became a well-established treatment paradigm after the publication of a longitudinal study of 1,355 patients from Mount Sinai and Massachusetts General Hospital.4 This study demonstrated that females less than 40 years old with moderate-to-severe generalized non-thymomatous MG who underwent thymectomy had significant (38% total remission, 51% improvement in symptoms) and sustained benefit.4
The only controlled randomized thymectomy trial was recently published in 2016. This was a multicenter trial that compared transsternal thymectomy plus prednisone with prednisone alone.5 126 patients were included under the following criteria: age 18–65, non-thymomatous MG, disease duration < 5 years, MGFA class II–IV, and elevated serum acetylcholine-receptor antibody. The thymectomy group demonstrated higher improvement in Quantitative Myasthenia Gravis scores and less immunosuppression requirement over a 3-year follow-up. Questions still to be answered are whether these benefits are sustained over longer periods of time, whether less invasive surgical approaches offer the same benefits, and whether these benefits can be seen without concurrent treatment with prolonged high-dose steroids.
Operative morbidity and mortality for thymectomy is 20% and 1%, respectively.6,7 Need for postoperative ventilation in one comparison study was 4% after VATS thymectomy and 16% after transsternal thymectomy.8 The most recent international consensus guidelines for management of MG recommend that9 (1) for patients with non-thymomatous, generalized MG, complete thymectomy is performed as an elective procedure to avoid or minimize immunosuppressive treatment; (2) all patients with thymomatous MG should undergo complete thymectomy, and incompletely resected thymomas should be treated with adjuvant chemotherapy and/or radiation; (3) less-invasive approaches to thymectomy (thoracoscopic, robotic) appear to yield similar results to more aggressive approaches, although this has not been shown in randomized controlled trials.
The patient in this case had postoperative bleeding and was taken back to the operating room on postoperative day 1 for exploration. After adequate monitoring, access, and resuscitation was established, the patient was intubated with a double-lumen endotracheal tube, and the patient was placed in the left lateral decubitus position. The right chest was entered via the previous thoracotomy incisions. About 1 L of hematoma was evacuated. Bleeding was identified at the sternal side of the internal mammary vein. This was controlled with suture ligation. The remainder of the patient’s postoperative course was unremarkable. She is currently weaning off steroids and having improved muscle strength. Final pathology demonstrated typical carcinoid tumor with 1 positive station 12 lymph node. The thymus specimen had fatty replacement with no thymic tissue identified.
Thymectomy is ultimately the most appealing form of MG treatment because it avoids the need for long-term commitment to immunosuppression or steroids. Advances in immunosuppressive drugs and emerging applications of techniques such as hematopoietic stem cell transplantation may be part of MG treatment in the future.10
Treatment for typical carcinoid tumors consists of complete resection and lymph node sampling. A lymph node in the fissure showed metastatic carcinoid tumor. Given her comorbidity, the extent of surgical resection is adequate. Radical lymph node dissection may have been an option for a healthier patient. Observation by computed tomography is a satisfactory management for our patient.
Disclosures
We have nothing to disclose.
Statement of Consent
The patient referred to in this video article has given their informed consent to be filmed and is aware that information and images will be published online.
References
- Jaretzki A III, Barohn RJ, Ernstoff RM, et al; Task Force of Medical Scientific Advisory Board of Myasthenia Gravis Foundation of America. Myasthenia gravis: recommendations for clinical research standards. Ann Thorac Surg. 2000;70(1):327-334. doi:10.1016/S0003-4975(00)01595-2.
- Blalock A, Mason MF, Morgan HJ, Riven SS. Myasthenia gravis and tumors of the thymic region: report of a case in which the tumor was removed. Ann Surg. 1939;110(4):544-561. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1391425/.
- Kirschner PA. Alfred Blalock and thymectomy for myasthenia gravis. Ann Thorac Surg. 1987;43(3):348-349. doi:10.1016/S0003-4975(10)60635-2.
- Perlo VP, Poskanzer DC, Schwab RS, Viets HR, Osserman KE, Genkins G. Myasthenia gravis: evaluation of treatment in 1,355 patients. Neurology. 1966;16(5):431-439. doi:10.1212/WNL.16.5.431.
- Wolfe GI, Kaminski HJ, Aban IB, et al. Randomized trial of thymectomy in myasthenia gravis. N Engl J Med. 2016;375(6):511-522. doi:10.1056/NEJMoa1602489.
- Bachmann K, Burkhardt D, Schreiter I, et al. Long-term outcome and quality of life after open and thoracoscopic thymectomy for myasthenia gravis: analysis of 131 patients. Surg Endosc. 2008;22(11):2470-2477. doi:10.1007/s00464-008-9794-2.
- Gronseth GS, Barohn RJ. Practice parameter: thymectomy for autoimmune myasthenia gravis (an evidence-based review). Neurology. 2000;55(1):7-15. doi:10.1212/WNL.55.1.7.
- Meyer DM, Herbert MA, Sobhani NC, et al. Comparative clinical outcomes of thymectomy for myasthenia gravis performed by extended transsternal and minimally invasive approaches. Ann Thorac Surg. 2009;87(2):385-391. doi:10.1016/j.athoracsur.2008.11.040.
- Sanders DB, Wolfe GI, Benatar M, et al. International consensus guidance for management of myasthenia gravis: executive summary. Neurology. 2016;87(4):419-425. doi:10.1212/WNL.0000000000002790.
- Bryant A, Atkins H, Pringle CE, et al. Myasthenia gravis treated with autologous hematopoietic stem cell transplantation. JAMA Neurol. 2016;73(6):652-658. doi:10.1001/jamaneurol.2016.0113.
Cite this article
Madariaga ML, Gaissert HA. Combined thymectomy and right lower lobe pulmonary wedge resection by thoracoscopy. J Med Insight. 2024;2024(181). doi:10.24296/jomi/181.
