
Hip Arthroscopy with Acetabular Osteoplasty and Labral Repair
Main Text
Table of Contents
Hip arthroscopy with femoral neck or acetabular osteoplasty with or without labral repair can be used for treatment of femoroacetabular impingement (FAI). Patients may present with insidious onset of hip pain and mechanical symptoms and pain worse with activity and sitting. On physical exam hip flexion and internal rotation may be reduced and anterior impingement testing will produce groin pain in the majority of patients with FAI. Imaging may demonstrate lesions responsible for cam-type or pincer-type impingement, and MRI may demonstrate labral tear or cartilaginous lesions. Arthroscopic surgical treatment is indicated for patients who have failed conservative treatment.
The patient is a 39-year-old female with significant right hip pain that persists despite conservative treatment with non-impact loading exercise, activity modification, and steroid injection. She is most bothered by getting out of deep chairs and pivoting activities. She had an MRI showing labral tear.
- Describe the onset of symptoms. Was it insidious or was there a preceding event?
- What is the location of pain?
- What is the quality of the pain? Are there any mechanical symptoms, such as a pop, snatch, catch, lock, or subluxation/instability?
- Is there exacerbation with sitting?
- Is pain activity-related?
- What relieves the pain?
- Do you walk with a limp?
- Do you have limitations to walking a distance or climbing stairs?
- Hip range of motion may be similar in the affected and unaffected hip.
- Assess flexion and internal rotation, comparing the affected and unaffected hip. The unaffected hip may exhibit reduced flexion and internal rotation or pain with range of motion.
- Assess for Trendelenburg sign by having patient stand on one leg on the affected side. The test is positive if the pelvis drops on the contralateral side. This occurs in 33% of patients with femoroacetabular impingement (FAI).
- Perform anterior impingement test by passively flexing the adducted hip and slowly internally rotating. This test reproduces anterior groin pain in 88% of patients with FAI.
- Perform FABER (flexion-abduction-external rotation) test.
- Perform resisted straight leg raise.
- Perform log roll test. Pain is reproduced in 30% of patient with FAI with log roll test.
- Perform posterior impingement test by placing the hip in extension and external rotation. Hip pain is reproduced in 21% of patients with FAI with posterior impingement test.
- Perform a complete exam of the affected limb and lumbar spine to rule out bursitis, nerve entrapment, and referred pain.1, 2
An AP pelvis view allows comparison of affected and unaffected femora. Assess symmetry to ensure that a true AP view has been captured. This can be assessed by checking that the coccyx overlaps the symphysis pubis, with no more than 2 cm of separation between the two structures. The joint should be assessed for reduction in joint space and degenerative changes. Compare the anterolateral neck contour with the unaffected side. Lack of superior neck concavity indicates reduced head-neck offset. Flat or increased radius of anterosuperior or anterior head indicates an aspherical head. Several measurements may be analyzed:
- Lateral Center Edge Angle: the angle formed by a vertical line drawn from the center of the femoral head and a line drawn from the lateral rim to the center of the head. An angle less than 20 degrees indicates dysplasia.
- Acetabular Index: the angle formed by the acetabular roof or sourcil. An angle greater than 10 degrees indicates dysplasia.
- Acetabular Version: traces lines from anterolateral acetabular edge along anterior and posterior projections of acetabular rim. An anterior wall that is more lateral than the posterior wall (“posterior wall sign”) indicates retroversion. An anterior wall that crosses the posterior wall (“cross-over sign”) indicates bony excess at anterior rim and relative retroversion.
- A cross-table lateral view is important for assessment of FAI, allowing a view of the anterolateral femoral neck.
- Alpha-angle: Formed between a line along the midline of the femoral neck and a line from the center of the femoral head to the point where excess bone deviates from normal femoral head sphericity. An angle greater than 60 degrees indicates FAI.
- Head-Neck Offset: Begin with a line bisecting longitudinal axis of femoral neck. Draw a parallel line that is tangential to the anterior aspect of the femoral neck and measure the distance to a parallel line tangential to the anterior femoral head. Normal distance is greater than 9 mm or a ratio to head diameter greater than 0.17.
MRI and CT can be used for further assessment of the acetabulum and proximal femur. These studies may provide superior assessment of acetabular version and soft tissue impingement or help with preoperative planning. MR Arthrogram may also assist with diagnosis of a cam lesion of the femoral neck, assess the labrum, or cartilage. Radial sequencing is best, an abnormal labrum will appear blunted or with increased signal at its base.3, 4 Pincer impingement, due to acetabular retroversion, will initially show labral failure followed by small, thin lesions to the posteroinferior acetabular cartilage as a result of a contracoup mechanism.5 This may be redemonstrated with a cross-over sign, the posterior wall sign, or a negative sourcil angle on radiographs. MRI will demonstrate blunted labrum, kissing lesion on femoral neck, wear of the posterior acetabular cartilage, or a retroverted acetabulum. Cam impingement, due to lesions of the femoral neck demonstrates initial failure of the cartilage followed by labral tearing. Assessing for decreased head-neck offset on the lateral x-ray, excess bone contours on the femoral neck, and an increased alpha-angle may aid in the diagnosis. On MRI the labrum may demonstrate tearing at its base, an abnormal femoral head-neck contour may be evident, or cartilage delamination may be evident. Patients will present with both cam and pincer impingement in 80% of cases, though one form is usually dominant.2
FAI is due to either a cam impingement, so-called “pistol grip deformity,” or pincer impingement, due to excess acetabular coverage. Etiology of cam impingement is unclear, but the reduction in femoral neck offset can cause hip pain and eventually lead to labral tears and chondral damage over time. Decreased femoral head-to-neck diameter ratio allows the femoral neck to abut on the anterior acetabulum and labrum in deep hip flexion. Chronic, repetitive impingement may lead to arthritic changes or labral tears in the presence of minor or altogether absent trauma.6
Initial non-surgical management for FAI includes activity modification and anti-inflammatory medication. Progression to surgical treatment should be considered for patients who fail conservative management. Surgical treatment of femoral neck lesions or labral tears may be treated by open or arthroscopic debridement and labral repair or resection. Indications for open treatment include non-spherical femoral head, decreased head-neck offset, pincer impingement, and posterior hip impingement lesions. The Bernese periacetabular osteotomy is an open acetabular reorientation procedure with the goal of decreasing acetabular retroversion. Chondral injuries of the acetabulum may be treated by chondroplasty, drilling, or microfracture, which aim to stimulate fibrocartilage regrowth. Acetabular anteversion and posterior osteophyte impingement may be treated with rim excision of the acetabulum. Arthroscopic clinical outcomes appear similar to open surgical clinical outcomes for the treatment of FAI.2, 3
Surgical repair for FAI seeks to return adequate joint space to allow hip range of motion without abutment of the femoral head or neck against the acetabulum. Excision of the lesions that reduce this space is performed to potentially slow the degenerative process and resolve impingement pain and other symptoms. Arthroscopy provides a less-invasive alternative to the traditional open surgery with similar clinical outcomes.4, 7
Patients should be aware that the degree of chondral damage at the time of the procedure correlates with the expected outcome. Older patients and those with relatively less joint space at the time of intervention are more likely to require subsequent total hip replacement. Increased satisfaction is observed in patients with ≥ 2 mm and those treated with repair of damaged labrum.8 A relative contraindication, therefore, is severe joint space narrowing (< 2 mm). Chondral damage of the femoral head indicates advanced disease and is associated with worse outcomes. Complications may result from several aspects of arthroscopic repair of FAI. Portal placement in proximity to the superior gluteal or femoral neurovascular bundles, or the lateral femoral cutaneous nerve can put these structures at risk during the procedure. Traction during the procedure can lead to sciatic nerve injury, which can be mitigated with gentle application of traction. Avascular necrosis risk increases with greater than 30% resection of the femoral neck. As with all excision procedures, fracture may result from the removal of excess bone.4
 Preoerative AP Pelvis
Preoerative AP Pelvis Preoperative AP Right Hip
Preoperative AP Right Hip Preoperative Lateral Right Hip
Preoperative Lateral Right Hip Preoperative Sagittal MRI - T1
Preoperative Sagittal MRI - T1 Preoperative Sagittal MRI - T2
Preoperative Sagittal MRI - T2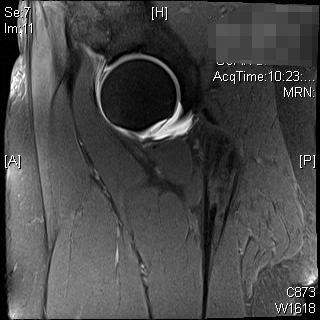 Preoperative Sagittal MRI - T2
Preoperative Sagittal MRI - T2FAI may represent an early step on the path to hip osteoarthritis. Arthroscopic treatment of FAI focuses on the repair of cam type lesions of the femoral neck and pincer type lesions of the acetabulum. The goal of these procedures is to alleviate symptoms and arrest the progression of osteoarthritic change in the hip. Compared with open surgery, these interventions have demonstrated similar clinical outcomes while utilizing a less-invasive approach. Patients should be aware that arthroscopic repair of FAI is most successful when employed for the treatment of early disease. Ideal candidates report reduced hip pain and clinical impingement tests demonstrate resolution of symptoms following the procedure in a majority of patients. Those undergoing the procedure with advanced degenerative change of the hip joint are far more likely to go on to have total hip replacement following arthroscopy. Investigators have also demonstrated improved clinical outcomes among patients treated with labrum-sparing procedures compared with those who have undergone labral-excising procedures.9, 10
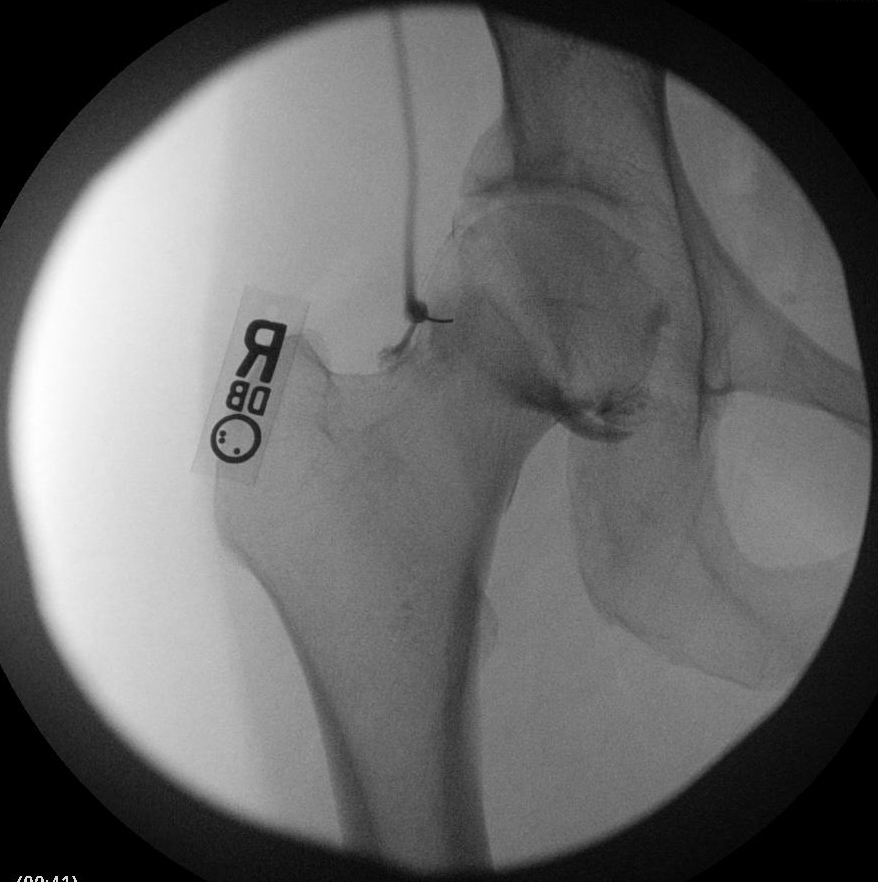 Intraoperative C-Arm AP Right Hip with contrast
Intraoperative C-Arm AP Right Hip with contrast Intraoperative C-Arm AP Right Hip with contrast
Intraoperative C-Arm AP Right Hip with contrast Intraoperative C-Arm AP Right Hip
Intraoperative C-Arm AP Right Hip Intraoperative Lateral Right hip
Intraoperative Lateral Right hip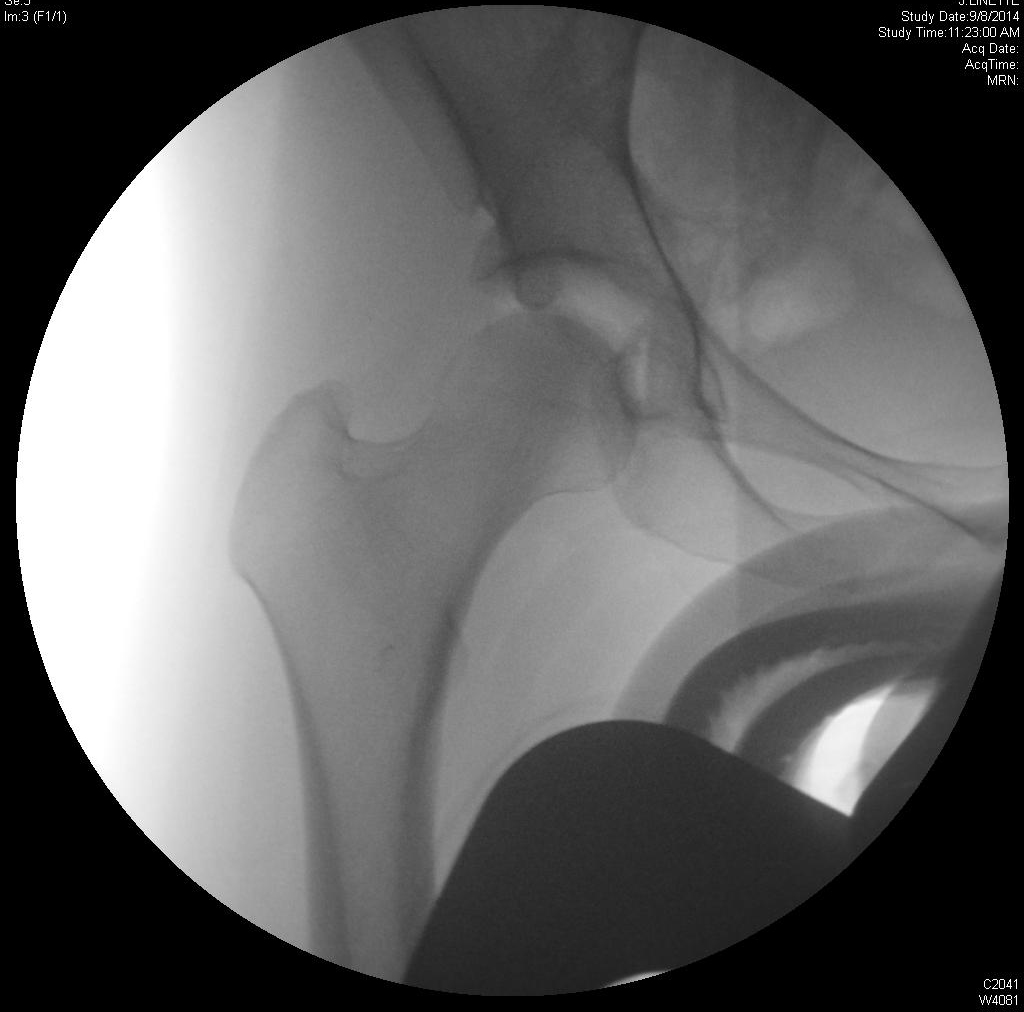 Intraoperative AP Right hip
Intraoperative AP Right hip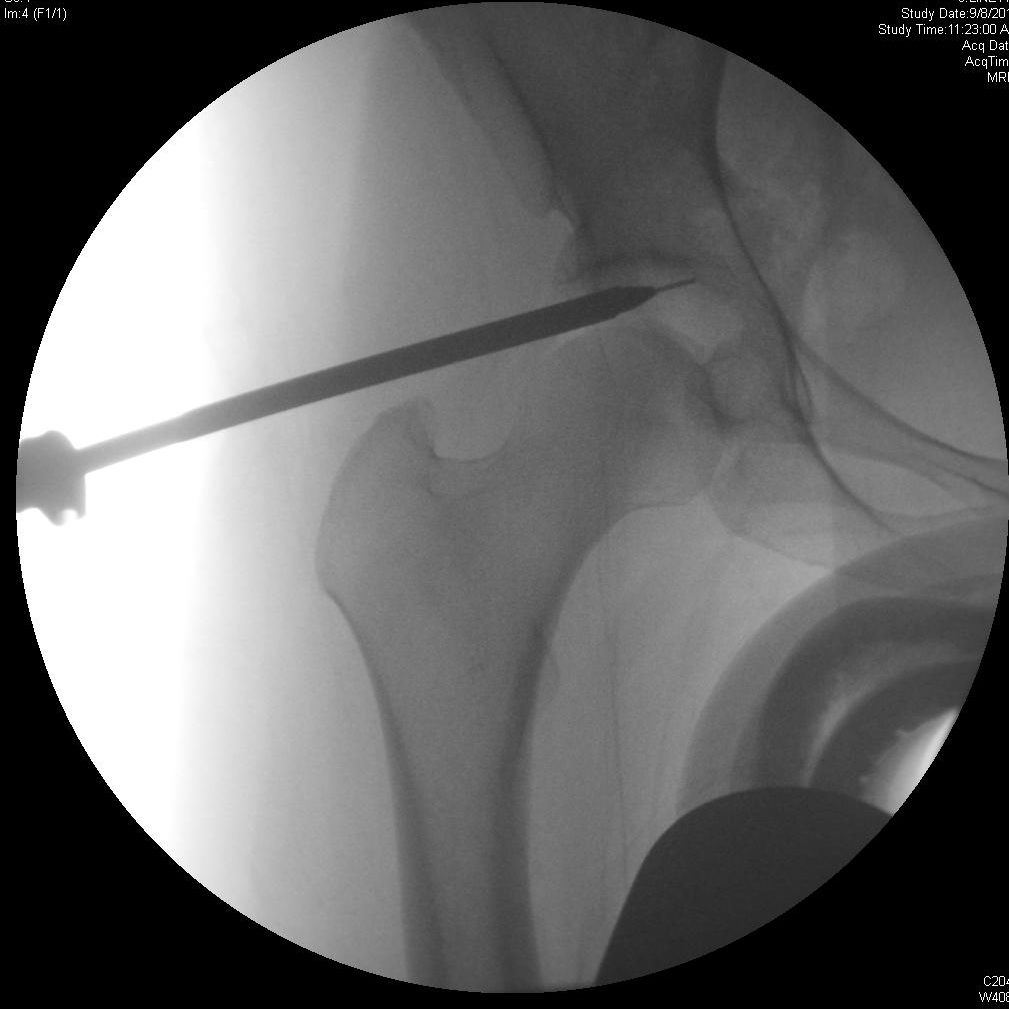 Intraoperative AP Right hip
Intraoperative AP Right hip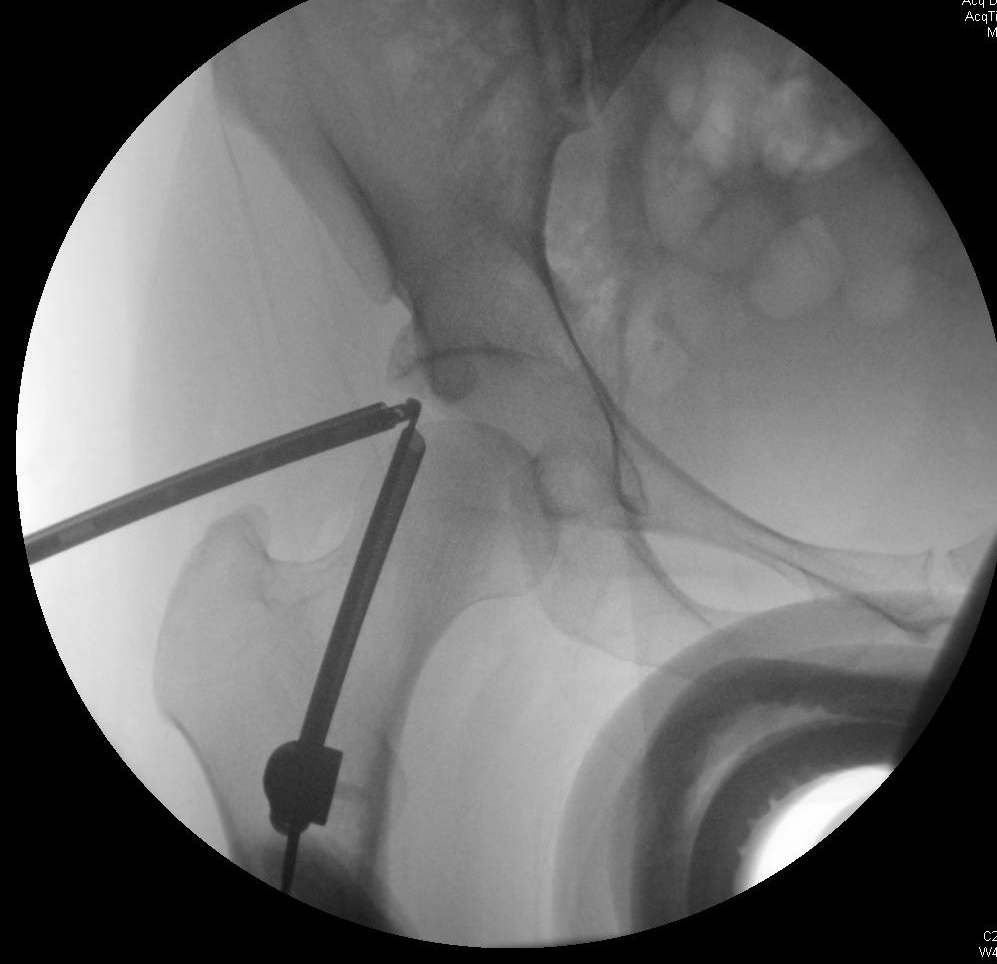 Intraoperative AP Right hip
Intraoperative AP Right hip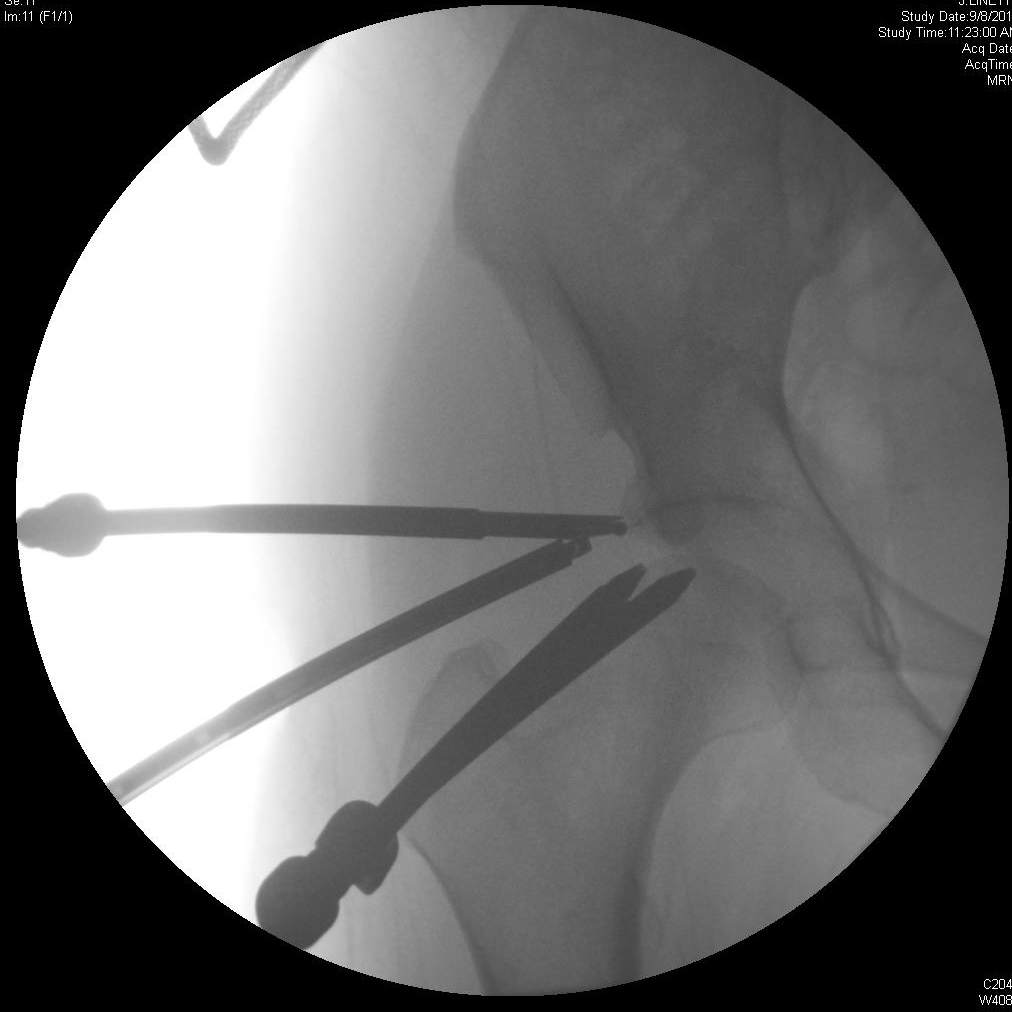 Intraoperative AP Right hip
Intraoperative AP Right hip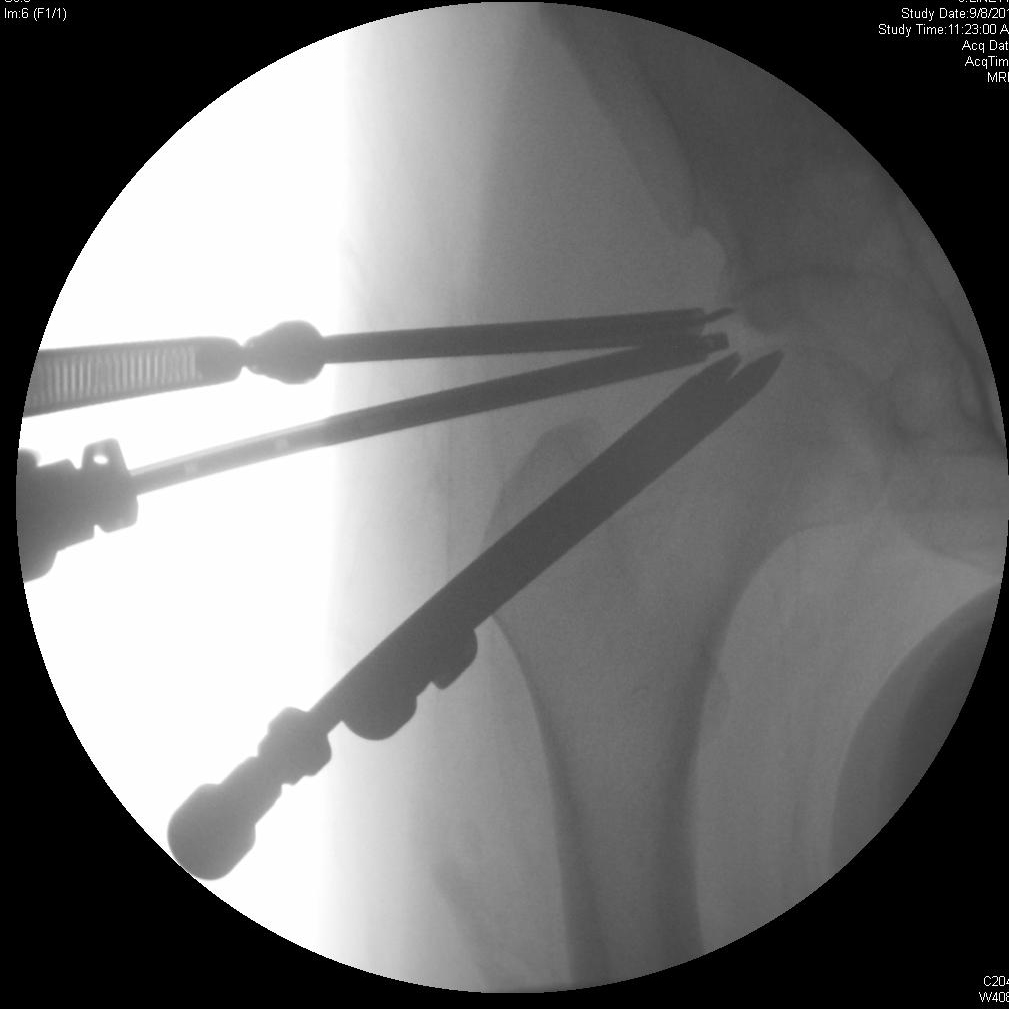 Intraoperative AP Right hip
Intraoperative AP Right hip Intraoperative AP Right hip
Intraoperative AP Right hipStudies have demonstrated improved clinical outcomes, resolution of symptoms, return to athletic performance, and elimination of clinical signs of impingement, which remain stable up to 3 years after treatment. Pain scores show a 74% reduction and patients rate their hips as “Excellent” or “Good” 75% of the time at 1 year postoperatively.7 Patients may experience optimal outcomes with adherence to a tiered postoperative rehabilitation routine that includes initially protected weight-bearing and range of motion.11
Future research should address long-term clinical outcomes with comparison between open surgical and arthroscopic approaches. In particular there should be studies to elucidate the patient or procedural factors associated with need to proceed to total hip replacement following initial surgical treatment of FAI. The success of subsequent hip arthroscopy also requires assessment.
The patient returned to clinic doing well without signs of infection, nerve injury, or joint instability following hip arthroscopy with labral repair and acetabular osteoplasty. She will remain non-weight bearing on crutches until six weeks postoperatively, at which time she will be advanced to weight bearing as tolerated.
- Knife Rasp, Smith and Nephew.
- 2.3 Bioraptor Osteoarticular suture anchors, Smith and Nephew.
- #2 FiberWire sutures, Arthrex.
The authors have no disclosures to make.
Informed consent was obtained from the patient to be featured in this video article. The patient is aware that it will be available on the internet. A copy of the consent is maintained in her medical records.
References
- Clohisy JC, Knaus ER, Hunt DM, Lesher JM, Harris-Hayes M, Prather H. Clinical presentation of patients with symptomatic anterior hip impingement. Clin Orthop Relat Res. 2009;467(3):638-644. doi:10.1007/s11999-008-0680-y.
- Guanche CA, Bare AA. Arthroscopic treatment of femoroacetabular impingement. Arthroscopy. 2006;22(1):95-106. doi:10.1016/j.arthro.2005.10.018.
- Ilizaliturri VM Jr, Orozco-Rodriguez L, Acosta-Rodríguez E, Camacho-Galindo J. Arthroscopic treatment of cam-type femoroacetabular impingement: preliminary report at 2 years minimum follow-up. J Arthroplasty. 2008;23(2):226-234. doi:10.1016/j.arth.2007.03.016.
- Philippon MJ, Stubbs AJ, Schenker ML, Maxwell RB, Ganz R, Leunig M. Arthroscopic management of femoroacetabular impingement: osteoplasty technique and literature review. Am J Sports Med. 2007;35(9):1571-1580. doi:10.1177/0363546507300258.
- Maheshwari AV, Malik A, Dorr LD. Impingement of the native hip joint. J Bone Joint Surg Am. 2007;89(11):2508-2518. doi:10.2106/JBJS.F.01296.
- Tanzer M, Noiseux N. Osseous abnormalities and early osteoarthritis: the role of hip impingement. Clin Orthop Relat Res. 2004;429:170-177. doi:10.1097/01.blo.0000150119.49983.ef.
- Larson CM, Giveans MR. Arthroscopic management of femoroacetabular impingement: early outcomes measures. Arthroscopy. 2008;24(5):540-546. doi:10.1016/j.arthro.2007.11.007.
- Philippon MJ, Briggs KK, Yen YM, Kuppersmith DA. Outcomes following hip arthroscopy for femoroacetabular impingement with associated chondrolabral dysfunction: minimum two-year follow-up. J Bone Joint Surg Br. 2009;91(1):16-23. doi:10.1302/0301-620X.91B1.21329.
- Larson CM, Giveans MR. Arthroscopic debridement versus refixation of the acetabular labrum associated with femoroacetabular impingement. Arthroscopy. 2009;25(4):369-376. doi:10.1016/j.arthro.2008.12.014.
- Kelly BT, Weiland DE, Schenker ML, Philippon MJ. Arthroscopic labral repair in the hip: surgical technique and review of the literature. Arthroscopy. 2005;21(12):1496-1504. doi:10.1016/j.arthro.2005.08.013.
- Stalzer S, Wahoff M, Scanlan M. Rehabilitation following hip arthroscopy. Clin Sports Med. 2006;25(2):337-357. doi:10.1016/j.csm.2005.12.008.
Cite this article
Martin SD. Hip arthroscopy with acetabular osteoplasty and labral repair. J Med Insight. 2023;2023(14). doi:10.24296/jomi/14.
